
Abstract
Purpose
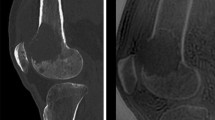
Osseous metastases often undergo an osteoblastic healing response following chemotherapy. The purpose of our study was to demonstrate the quantitative CT changes in attenuation of osseous metastases before and after chemotherapy.
Materials and methods
Our study was IRB approved and HIPAA compliant. Our cohort consisted of 86 consecutive cancer patients with contrast-enhanced CTs before and 14 ± 2 (12–25) months after initiation of chemotherapy (60 ± 11 years, 36 males, 50 females). The average and maximum metastasis attenuations were measured in Hounsfield units (HU) by two readers. Treatment effects were assessed using paired t-tests and Fisher exact tests. Intraclass correlation coefficients (ICCs) were calculated. Patient records were reviewed to determine the patient’s clinical status (worse, unchanged, or improved) at the time of follow-up CT.
Results
The distribution of lesion types was as follows: lytic (30/86, 35%), blastic (43/86, 50%), and mixed lytic-blastic (13/86, 15%). There was a significant increase in average and maximum CT attenuation of metastases following chemotherapy for all patients, which remained statistically significant when stratified by lesion type, clinical status (worsening or improving/stable), cancer type (breast, lung), and radiation therapy (P < 0.05). In a subgroup of patients whose osseous metastases decreased in average attenuation (14/86, 16%), more patients had a worse clinical status (11/14, 79%) (P = 0.02). ICC was almost perfect for average attenuation and substantial for maximum attenuation.
Conclusion
Quantitative assessment of osseous metastatic disease using CT attenuation measurements demonstrated a statistically significant increase in attenuation more than 12 months after initiation of chemotherapy.





Similar content being viewed by others


References
Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res. 2006;12:6243s–9s.
Li S, Peng Y, Weinhandl ED, Blaes AH, Cetin K, Chia VM, et al. Estimated number of prevalent cases of metastatic bone disease in the US adult population. Clin Epidemiol. 2012;4:87–93.
Söderlund V. Radiological diagnosis of skeletal metastases. Eur Radiol. 1996;6:587–95.
Clemons M, Gelmon KA, Pritchard KI, Paterson AHG. Bone-targeted agents and skeletal-related events in breast cancer patients with bone metastases: the state of the art. Curr Oncol. 2012;19:259–68.
Hamaoka T, Madewell JE, Podoloff DA, Hortobagyi GN, Ueno NT. Bone imaging in metastatic breast cancer. J Clin Oncol. 2004;22:2942–53.
Basu S, Alavi A. Defining co-related parameters between “metabolic” flare and “clinical”, “biochemical”, and “osteoblastic” flare and establishing guidelines for assessing response to treatment in cancer. Eur J Nucl Med Mol Imaging. 2007;34:441–3.
Janicek MJ, Hayes DF, Kaplan WD. Healing flare in skeletal metastases from breast cancer. Radiology. 1994;192:201–4.
Lemieux J, Guimond J, Laberge F, St-Pierre C, Cormier Y. The bone scan flare phenomenon in non-small-cell lung cancer. Clin Nucl Med. 2002;27:486–9.
Vogel CL, Schoenfelder J, Shemano I, Hayes DF, Gams RA. Worsening bone scan in the evaluation of antitumor response during hormonal therapy of breast cancer. J Clin Oncol. 1995;13:1123–8.
Cosolo W, Morstyn G, Arkles B, Zimet AS, Zalcberg JR. Flare responses in small cell carcinoma of the lung. Clin Nucl Med. 1988;13:13–6.
Pollen JJ, Witztum KF, Ashburn WL. The flare phenomenon on radionuclide bone scan in metastatic prostate cancer. AJR Am J Roentgenol. 1984;142:773–6.
Pollen JJ, Shlaer WJ. Osteoblastic response to successful treatment of metastatic cancer of the prostate. AJR Am J Roentgenol. 1979;132:927–31.
DeMartini AL, Buzdar AU, Blumenschein GR. Osteoblastic metastatic disease as a therapeutic response to adjuvant chemotherapy in breast cancer. J Surg Oncol. 1983;23:32–4.
Dehdashti F, Flanagan FL, Mortimer JE, Katzenellenbogen JA, Welch MJ, Siegel BA. Positron emission tomographic assessment of “metabolic flare” to predict response of metastatic breast cancer to antiestrogen therapy. Eur J Nucl Med. 1999;26:51–6.
Amoroso V, Pittiani F, Grisanti S, Valcamonico F, Simoncini E, Ferrari VD, et al. Osteoblastic flare in a patient with advanced gastric cancer after treatment with pemetrexed and oxaliplatin: implications for response assessment with RECIST criteria. BMC Cancer. 2007;7:94.
Stattaus J, Hahn S, Gauler T, Eberhardt W, Mueller SP, Forsting M, et al. Osteoblastic response as a healing reaction to chemotherapy mimicking progressive disease in patients with small cell lung cancer. Eur Radiol. 2009;19:193–200.
Messiou C, Cook G, Reid AHM, Attard G, Dearnaley D, de Bono JS, et al. The CT flare response of metastatic bone disease in prostate cancer. Acta Radiol. 2011;52:557–61.
Quattrocchi CC, Santini D, Dell’aia P, Piciucchi S, Leoncini E, Vincenzi B, et al. A prospective analysis of CT density measurements of bone metastases after treatment with zoledronic acid. Skelet Radiol. 2007;36:1121–7.
Guise TA, Mundy GR. Cancer and bone. Endocr Rev. 1998;19:18–54.
Sosnoski DM, Krishnan V, Kraemer WJ, Dunn-Lewis C, Mastro AM. Changes in cytokines of the bone microenvironment during breast cancer metastasis. Int J Breast Cancer. 2012;2012:160265.
Kinder M, Chislock E, Bussard KM, Shuman L, Mastro AM. Metastatic breast cancer induces an osteoblast inflammatory response. Exp Cell Res. 2008;314:173–83.
Bussard KM, Venzon DJ, Mastro AM. Osteoblasts are a major source of inflammatory cytokines in the tumor microenvironment of bone metastatic breast cancer. J Cell Biochem. 2010;111:1138–48.
David RG. Role of stromal-derived cytokines and growth factors in bone metastasis. Cancer. 2003;97:733–8.
Yamashita Y, Aoki T, Hanagiri T, Yoshii C, Mukae H, Uramoto H, et al. Osteosclerotic lesions in patients treated with gefitinib for lung adenocarcinomas: a sign of favorable therapeutic response. Skelet Radiol. 2012;41:409–14.
Simeone FJ, Bennett DL, Chang CY, Huang AJ, Kattapuram SV, Bredella MA, et al. Retrospective analysis of intravertebral collateral enhancement in patients with central venous obstruction. Skelet Radiol. 2016;45:163–8.
O’Sullivan GJ, Carty FL, Cronin CG. Imaging of bone metastasis: an update. World J Radiol. 2015;7:202–11.
Bäuerle T, Semmler W. Imaging response to systemic therapy for bone metastases. Eur Radiol. 2009;19:2495–507.
Ulano A, Bredella MA, Burke P, Chebib I, Simeone FJ, Huang AJ, et al. Distinguishing untreated osteoblastic metastases from enostoses using CT attenuation measurements. AJR Am J Roentgenol. 2016:1–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
None
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was waived for individual participants included in the study. The study was approved by the local Institutional Review Board (IRB) and is HIPAA compliant.
Rights and permissions
About this article

Cite this article
Chang, C.Y., Simeone, F.J., Torriani, M. et al. Quantitative contrast-enhanced CT attenuation evaluation of osseous metastases following chemotherapy. Skeletal Radiol 46, 1385–1395 (2017). https://doi.org/10.1007/s00256-017-2706-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-017-2706-6