
Abstract
Purpose
To evaluate the feasibility and intra- and interobserver agreement of CBCT arthrography of wrist ligaments, triangular fibrocartilaginous complex (TFCC), and to assess the sensitivity (SE), specificity (SP), accuracy (ACC), and positive and negative predictive value (PPV, NPV) of CBCT arthrography in the diagnosis of scapholunate (SLL) and lunotriquetral (LTL) ligament tears, TFCC, and cartilage abnormalities of the scaphoid and lunate with their corresponding radial surfaces (scaphoid and lunate fossa) using a novel, mobile, dedicated extremity CBCT scanner.
Materials and methods
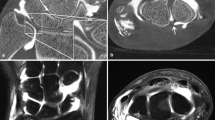
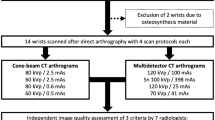
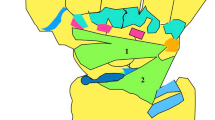
Fifty-two consecutively enrolled subjects (26 M, 26 F, mean age 38 years, range 18–66 years) with suspected wrist ligament tears underwent CBCT-arthrography before normally scheduled MR arthrography.An extremity CBCT was used for imaging with isotropic voxel size of 0.4 × 0.4 × 0.4 mm3. Subsequent routine 1.5 T MRI was performed using a dedicated wrist coil.Two observers reviewed the anonymized CBCT images twice for contrast enhancement (CE) and technical details (TD), for tears of the SLL, LTL, and TFCC. Also, cartilage abnormalities of the scaphoid and lunate with their corresponding radial surfaces (scaphoid and lunate fossa) were evaluated. Inter- and intraobserver agreement was determined using weighted kappa statistics. Since no surgery was performed, MRI served as a reference standard, and SE and SP, ACC, PPV, and NPV were calculated.
Results
Intra- and interobserver kappa values for both readers (reader 1/reader 2; first reading/second reading) with 95 % confidence limits were: CE 0.54 (0.08–1.00)/ 0.75 (0.46–1.00); 0.73 (0.29–1.00)/ 0.45 (0.07–0.83), TD 0.53 (0.30–0.88)/ 0.86 (0.60–1.00); 0.56 (0.22–0.91)/ 0.67 (0.37–0.98), SLL 0.59 (0.25–0.93)/ 0.66 (0.42–0.91); 0.31 (0.06–0.56)/ 0.49 (0.26–0.73), LTL 0.83 (0.66–1.00)/ 0.68 (0.46–0.91); 0.90 (0.79–1.00)/ 0.48 (0.22–0.74); TFCC (0.72–1.00)/ (0.79–1.00); 0.65 (0.43–0.87)/ 0.59 (0.35–0.83), radius (scaphoid fossa) 0.45 (0.12–0.77)/ 0.64 (0.31–0.96); 0.58 (0.19–0.96)/ 0.38 (0.09–0.66), scaphoid 0.43 (0.12–0.74)/ 0.76 (0.55–0.96); 0.37 (0.00–0.75)/ 0.32 (0.04–0.59), radius (lunate fossa) 0.68 (0.36–1.00)/ 0.42 (0.00–0.86); 0.62 (0.29–0.96)/ 0.51 (0.12–0.91), and lunate 0.53 (0.16–0.90)/ 0.68 (0.44–0.91); 0.59 (0.29–0.88)/ 0.42 (0.00–0.84), respectively.
The overall mean accuracy was 82–92 % and specificity was 81–94 %. Sensitivity for LTL and TFCC tears was 76–83, but for SLL tears it was 58 %. For cartilage abnormalities, the accuracy and negative predictive value were high, 90–98 %.
Conclusions
A dedicated CBCT extremity scanner is a new method for evaluating the wrist ligaments and radiocarpal cartilage. The method has an overall accuracy of 82–86 % and specificity 81–91 %. For cartilage abnormalities, the accuracy and negative predictive value were high.







Similar content being viewed by others
References
Zlatkin MB, Chao PC, Osterman AL, Schnall MD, Dalinka MK, Kressel HY. Chronic wrist pain: evaluation with high-resolution imaging. Radiology. 1989;173:723–9.
Smith DK. MR imaging of normal and injured wrist ligaments. Magn Reson Imaging Clin N Am. 1995;3:229–48.
Golimbu CN, Firooznia H, Melone CP, Rafii M, Weinreb J, Leber C. Tears of the triangular fibrocartilage of the wrist: MR imaging. Radiology. 1989;173:731–3.
Hobby JL, Tom BD, Bearcroft PW, Dixon AK. Magnetic resonance imaging of the wrist: diagnostic performance statistics. Clin Radiol. 2001;56:50–7.
Haims AH, Moore AE, Schweitzer ME, Morrison WB, Deely D, Culp RW, et al. MRI in the diagnosis of cartilage injury in the wrist. Am J Roentgenol. 2004;182:1267–70.
Moser T, Dosch JC, Moussaoui A, Dietemann JL. Wrist ligament tears: evaluation of MRI and combined MDCT and MR arthrography. Am J Roentgenol. 2007;188:1278–86.
Cerezal L, de Dios Berná-Mestre J, Canga A, et al. MR and CT arthrography of the wrist. Semin Musculoskelet Radiol. 2012;16:27–41.
Mozzo P, Procacci C, Tacconi A, et al. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. Eur Radiol. 1998;8:1558–64.
Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K. Development of compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol. 1999;28:245–8.
De Vos W, Casselman J, Swennen GRJ. Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: a systematic review of the literature. Int J Oral Maxillofac Surg. 2009;38:609–25.
Faccioli N, Foti G, Barillari M, Atzei A, Mucelli RP. Finger fractures imaging: accuracy of cone-beam computed tomography and multislice computed tomography. Skeletal Radiol. 2010;39:1087–95.
De Cock J, Mermuys K, Goubau J, van Petegem S, Houthoofdt B, Casselman JW. Cone-beam computed tomography: a new low-dose, high-resolution imaging technique of the wrist, presentation of three cases with technique. Skeletal Radiol. 2012;41:93–6.
Zbijewski W, De Jean P, Prakash P, et al. A dedicated cone-beam CT system for musculoskeletal extremities imaging: design, optimization, and initial performance characterization. Med Phys. 2011;38:4700–13.
Mattila KT, J. Kankare J, Kortesniemi M, et al. Cone beam CT for extremity imaging. EPOS Abstract, ECR 2011, Vienna March 3–7, 2011. doi:10.1594/ecr2011/C-0297.
Biswas D, Bible JE, Bohan M, Simpson AK, Whang PG, Grauer JN. Radiation exposure from musculoskeletal computerized tomographic scans. J Bone Joint Surg Am. 2009;91:1882–9.
Landis JR, Koch GG. The measurement of observer agreement for categorial data. Biometrics. 1997;33:159–74.
Guggenberger R, Fischer MA, Hodler J, Pfammatter T, Andreisek G. Flat-panel CT-arthrography. Feasibility study and comparison to multidetector CT arthrography. Invest Radiol. 2012;47:312–8.
Zheng Z-Z, Shan H, Li X. Fat-suppressed 3D T1-weighted gradient-echo imaging of the cartilage with a volumetric interpolated breath-hold examination. Am J Roentgenol. 2010;194:W414–9.
Heigl B, Kowarschik M. High-Speed Reconstruction for C-Arm Computed Tomography. In Proceedings of the 9th International Meeting on Fully Three-Dimensional Image Reconstruction in Radiology and Nuclear Medicine, pp. 25–28, Lindau, Germany, July 2007.
Tsiklakis K, Donta C, Gavala S, Karayianni K, Kamenopoulou V, Hourdakis CJ. Dose reduction in maxillofacial imaging using low-dose cone-beam CT. Eur J Radiol. 2005;56:413–7.
Roberts JA, Drage NA, Davies J, Thomas DW. Effective dose from cone-beam CT examinations in dentistry. Br J Radiol. 2009;82:35–40.
Koong B. Cone-beam imaging: is this the ultimate imaging modality? Clin Oral Implants Res. 2010;21:1201–8.
Hart D, Wall BF. Radiation Exposure of the UK population from Medical and Dental X-ray Examinations; Report NRPB-W4; National Radiological Protection Board, UK; 2002.
Donker DK, Hasman A, van Geijn HP. Interpretation of low kappa values. Int J Biomed Comp. 1993;33:55–64.
Scheck RJ, Romagnolo A, Hierner R, Pfluger T, Wilhelm K, Hahn K. The carpal ligaments in MR arthrography of the wrist: correlation with standard MRI and wrist arthroscopy. J Magn Reson Imaging. 1999;9:468–74.
Omlor G, Jung M, Grieser T, Ludwig K. Depiction of the triangular fibro-cartilage in patients with ulnar-sided wrist pain: comparison of direct multi-slice CT arthrography and direct MR arthrography. Eur Radiol. 2009;19:147–51.
Acknowledgments
Sharon J. Kuong, MD, is acknowledged for her linguistic help.
Conflict of interest
The authors acknowledge that within the past 3 years they have received benefits which might result in a conflict of interest or the appearance of a conflict. Nature of benefit: Research Consultans (authors 1,3–5,7), employment (author 6).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Koskinen, S.K., Haapamäki, V.V., Salo, J. et al. CT arthrography of the wrist using a novel, mobile, dedicated extremity cone-beam CT (CBCT). Skeletal Radiol 42, 649–657 (2013). https://doi.org/10.1007/s00256-012-1516-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-012-1516-0