
Abstract
Objective
The aim of the present study was to analyse magnetic resonance findings of intramuscular metastases (IM) in a relatively large series.
Materials and Methods
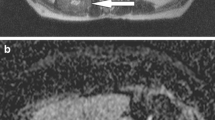
From January 2000 to January 2010, 28 patients (207 metastases) were retrospectively identified in the radiological database of the Martin-Luther-University. Several different scanning protocols were used depending on the localisation of IM. In 12 patients diffusion-weighted (DW) images were obtained with a multi-shot SE-EPI sequence. Apparent diffusion coefficient (ADC) maps were also calculated. Furthermore, fusion images were manually generated between the DW and half-Fourier acquisition single-shot turbo spin echo (HASTE) images.
Results
On T2-weighted images, 97% of the recognised IM were hyperintense in comparison to unaffected musculature, and 3% were mixed iso- to hyperintense. On T1-weighted images most IM (91%) were homogeneously isointense in comparison to muscle tissue, whereas 4% were hypointense, and 5% lightly hyperintense. ADC maps were calculated for 91 metastases ranging from 0.99 to 4.00 mm2s−1 (mean value 1.99 ± 0.66). ADC values of low (<1.5) signal intensity (SI) were identified in 26%, moderate SI (from 1.5 to 3.0) in 68%, and high SI (>3.0) in 6%. Of the IM that were investigated with contrast medium, 88.5% showed marked enhancement. It was homogeneous in 88% and heterogenous in 6%. Rim enhancement with central low attenuation was seen in 6%. There was no difference in enhancement characteristics with respect to ADC values or fusion patterns. Peritumoral enhancement was identified in 2.4%.
Conclusion
Magnetic resonance features of muscle metastases are relatively typical and consist of round or oval intramuscular masses with well-defined margins, marked enhancement, low or moderate ADC values, and moderate to high signal intensity on fusion images.



Similar content being viewed by others

References
Kurek J, Nouri S, Kannourakis G, Murphy M, Austin L. Leukemia inhibitory factor and interleukin-6 are produced by diseased and regenerating skeletal muscle. Muscle Nerve. 1996;19:1291–301.
Weiss L. Biomechanical destruction of cancer cells in skeletal muscle: a rate-regulator for hematogenous metastasis. Clin Exp Metastasis. 1989;5:483–91.
Seely S. Possible reasons for high resistance of muscle to cancer. Med Hypotheses. 1980;6:133–7.
Hasegawa S, Sakurai Y, Imazu H, et al. Metastasis to the forearm skeletal muscle from an adenocarcinoma of the colon: report of a case. Surg Today. 2000;30:1118–23.
Nabeyama R, Tanaka K, Matsuda S, Iwamoto Y. Multiple intramuscular metastases 15 years after radical nephrectomy in a patient with stage IV renal cell carcinoma. J Orthop Sci. 2001;6:189–92.
Willis RA. The spread of tumours in the human body. London: Butterworth; 1952.
Glockner DM, White LM, Sundaram M, McDonald DJ. Unsuspected metastases presenting as solitary soft tissue lesions: a fourteen-year review. Skeletal Radiol. 2000;29:270–4.
Surov A, Hainz M, Holzhausen HJ, Arnold D, Katzer M, Schmidt J, et al. Skeletal muscle metastases: primary tumours, prevalence, and radiological features. Eur Radiol. 2010;20:649–58.
Magee T, Rosenthal H. Skeletal muscle metastases at sites of documented trauma. AJR Am J Roentgenol. 2002;178:985–8.
Tuoheti Y, Okada K, Osanai T, et al. Skeletal muscle metastases of carcinomas: a clinicopathological study of 12 cases. Jpn J Clin Oncol. 2004;34:210–4.
O’Brien JM, Brennan DD, Taylor DH, et al. Skeletal muscle metastasis from uterine leiomyosarcoma. Skeletal Radiol. 2004;33:655–9.
Williams JB, Youngberg RA, Bui-Mansfield LT, Pitcher JD. MR imaging of skeletal muscle metastases. AJR Am J Roentgenol. 1997;168:555–7.
Lee BY, Choi JE, Park JM, et al. Various image findings of skeletal muscle metastases with clinical correlation. Skeletal Radiol. 2008;37:923–8.
Yoshioka H, Itai Y, Niitsu M, et al. Intramuscular metastasis from malignant melanoma: MR findings. Skeletal Radiol. 1999;28:714–6.
Sakamoto A, Yoshida T, Matsuura S, et al. Metastasis to the gluteus maximus muscle from renal cell carcinoma with special emphasis on MR features. World J Surg Oncol. 2007;5:88–92.
Nishie A, Stolpen AH, Obuchi M, Kuehn DM, Dagit A, Andresen K. Evaluation of locally recurrent pelvic malignancy: performance of T2- and diffusion-weighted MRI with image fusion. J Magn Reson Imaging. 2008;28:705–13.
Bauer A, Reiser MF. Diffusion-weighted imaging of the musculoskeletal system in humans. Skeletal Radiol. 2000;29:555–62.
Schnapauff D, Zeile M, Niederhagen MB, et al. Diffusion-weighted echo-planar magnetic resonance imaging for the assessment of tumor cellularity in patients with soft-tissue sarcomas. J Magn Reson Imaging. 2009;29:1355–9.
Einarsdóttir H, Karlsson M, Wejde J, Bauer HC. Diffusion-weighted MRI of soft tissue tumours. Eur Radiol. 2004;14(6):959–63.
Van Rijswijk CS, Kunz P, Hogendoorn PC, Taminiau AH, Doornbos J, Bloem JL. Diffusion-weighted MRI in the characterization of soft-tissue tumors. J Magn Reson Imaging. 2002;15:302–7.
Dudeck O, Zeile M, Pink D, et al. Diffusion-weighted magnetic resonance imaging allows monitoring of anticancer treatment effects in patients with soft-tissue sarcomas. J Magn Reson Imaging. 2008;27:1109–13.
Oka K, Yakushiji T, Sato H, Hirai T, Yamashita Y, Mizuta H. The value of diffusion-weighted imaging for monitoring the chemotherapeutic response of osteosarcoma: a comparison between average apparent diffusion coefficient and minimum apparent diffusion coefficient. Skeletal Radiol. 2010;39(2):141–6.
Fujii S, Matsusue E, Kanasaki Y, et al. Detection of peritoneal dissemination in gynecological malignancy: evaluation by diffusion-weighted MR imaging. Eur Radiol. 2008;18:18–23.
Suresh S, Saifuddin A, O’Donnell P. Lymphoma presenting as a musculoskeletal soft tissue mass: MRI findings in 24 cases. Eur Radiol. 2008;18:1628–34.
Eustace S, Winalski CS, McGowen A, Dorfman D. Skeletal muscle lymphoma. Observation at MR imaging. Skeletal Radiol. 1996;25:425–30.
Sundaram M. MR imaging of soft tissue tumors: an overview. Semin Musculoskelet Radiol. 1999;3:15–20.
Gaeta M, Mazziotti S, Minutoli F, et al. MR imaging findings of focal myositis: a pseudotumour that may mimic muscle neoplasm. Skeletal Radiol. 2009;38:571–8.
Conflict of interest
The authors declare that there is no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Surov, A., Fiedler, E., Voigt, W. et al. Magnetic resonance imaging of intramuscular metastases. Skeletal Radiol 40, 439–446 (2011). https://doi.org/10.1007/s00256-010-1018-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-010-1018-x