
Abstract
Objective
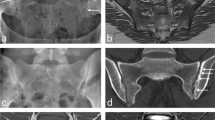
The “penumbra sign” on unenhanced T1-weighted MR sequences is thought to be helpful for discriminating subacute osteomyelitis from bone neoplasm. We sought to quantify the sensitivity and specificity of this sign for bone and soft tissue infection in a general referral population.
Design
Clinical coding was used to identify patients admitted to Middlemore Hospital (Auckland, New Zealand) between January 2000 and November 2003 with a diagnosis of either infection or neoplasm of the upper or lower limb who had undergone an MRI scan. One hundred and eighty-three patients were included in the study. Fifty-seven patients had bone or soft tissue infection. One hundred and twenty-six had a bone or soft tissue neoplasm. Relevant unenhanced T1-weighted images were selected for each patient, randomised and placed in a folder on the Hospital PACS system. Four reviewers were shown the original article describing the penumbra sign and then asked to look at the images in the folder stating whether the penumbra sign was present or absent.
Results
The average specificity and sensitivity of the penumbra sign for musculoskeletal infection was 96% (range 94–99%) and 27% (range 21–34%) respectively. Interobserver reliability was moderate to good with an average kappa score of 0.57 (range 0.50–0.62). For isolated soft tissue infection there was a higher sensitivity (54%, 33–83%) but with similar specificity (98%, 96–100%) and interobserver reliability (0.47, 0.33–0.58). Of the 11 out of 57 (19%) true positive penumbra signs identified by a consensus of three or more of the observers, all were subacute, chronic or acute on chronic infections.
Conclusions
The penumbra sign has a high specificity for musculoskeletal infection. This is also true for isolated soft tissue infection. The penumbra sign is helpful in differentiating neoplasm from infection and its presence in the setting of a high pretest probability is useful in making a diagnosis of infection.


Similar content being viewed by others

References
Willis RB, Rozencwaig R. Paediatric osteomyelitis masquerading as skeletal neoplasia. Paediatr Oncol 1996;27(3): 625–634.
Durbon M, Randall R, James M, Sudilovsky D, Zoger S. Ewing’s sarcoma masquerading as osteomyelitis. Clin Orthop Relat Res 1998;357(1): 176–185.
Chung T. Magnetic resonance imaging in acute osteomyelitis in children. Pediatr Infect Dis J 2002;21: 869–870.
Tehranzadeh J, Wong E, Wang F, Sadighpour M. Imaging of osteomyelitis in the mature skeleton. Radiol Clin North Am 2001;39(2): 223–250.
Erdman WA, Tamburro F, Jayson HT, Weatherall PT, Ferry KB, Peshock RM. Osteomyelitis: characteristics and pitfalls of diagnosis with MR imaging. Radiology 1991;180: 533–539.
Grey AM, Davies AM, Mangham DC, Grimer RJ, Ritchie DA. The ‘Penumbra Sign’ on T1-weighted MR imaging in subacute osteomyelitis: frequency, cause and significance. Clin Radiol 1998;53(8): 587–592.
Marui T, Yamamoto I, Akisue T, et al. Subacute osteomyelitis of long bones: Diagnostic usefulness of the Penumbra Sign on MRI. Clin Imaging 2002;26: 314–315.
Guermazi A, Mohr A, Genant HK. Brodie abscess: another type of chronic posttraumatic osteomyelitis. Eur Radiol 2003;13: 1750–1752.
Davies AM, Grimer R. The penumbra sign in subacute osteomyelitis. Eur Radiol 2005;15: 1268–1270.
Nguyen SL, Doyle AJ, Symmans PJ. Interstitial fluid and the hypoechoic wall: two sonographic signs of breast abscess. J Clin Ultrasound 2000;28(7): 319–324.
Hui CL, Naidoo P. Extramedullary fat fluid level on MRI as a specific sign for osteomyelitis. Australas Radiol 2003;47: 443–446.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McGuinness, B., Wilson, N. & Doyle, A.J. The “penumbra sign” on T1-weighted MRI for differentiating musculoskeletal infection from tumour. Skeletal Radiol 36, 417–421 (2007). https://doi.org/10.1007/s00256-006-0267-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-006-0267-1