
Abstract
Background
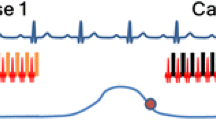
The benefits of cardiac magnetic resonance imaging (MRI) in the pediatric population must be balanced with the risk and cost of anesthesia. Segmented imaging using multiple averages attempts to avoid breath-holds requiring general anesthesia; however, cardiorespiratory artifacts and prolonged scan times limit its use. Thus, breath-held imaging with general anesthesia is used in many pediatric centers. The advent of free-breathing, motion-corrected (MOCO) cines by real-time re-binned reconstruction offers reduced anesthesia exposure without compromising image quality.
Objective
This study evaluates sedation utilization in our pediatric cardiac MR practice before and after clinical introduction of free-breathing MOCO imaging for cine and late gadolinium enhancement.
Materials and methods
In a retrospective study, patients referred for a clinical cardiac MR who would typically be offered sedation for their scan (n=295) were identified and divided into two eras, those scanned before the introduction of MOCO cine and late gadolinium enhancement sequences and those scanned following their introduction. Anesthesia use was compared across eras and disease-specific cohorts.
Results
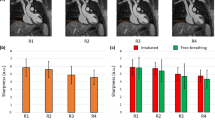
The incidence of non-sedation studies performed in children nearly tripled following the introduction of MOCO imaging (25% [pre-MOCO] to 69% [post-MOCO], P<0.01), with the greatest effect in patients with simple congenital heart disease. Eleven percent of the post-MOCO cohort comprised infants younger than 3 months of age who could forgo sedation with the combination of MOCO imaging and a “feed-and-bundle” positioning technique.
Conclusion
Implementation of cardiac MR with MOCO cine and late gadolinium enhancement imaging in a pediatric population is associated with significantly decreased sedation utilization.





Similar content being viewed by others

References
Fratz S, Chung T, Greil GF et al (2013) Guidelines and protocols for cardiovascular magnetic resonance in children and adults with congenital heart disease: SCMR expert consensus group on congenital heart disease. J Cardiovasc Magn Reson 15:51
Vincenti G, Monney P, Chaptinel J et al (2014) Compressed sensing single-breath-hold CMR for fast quantification of LV function, volumes, and mass. JACC Cardiovasc Imaging 7:882–892
Cross R, Olivieri L, O’Brien K et al (2016) Improved workflow for quantification of left ventricular volumes and mass using free-breathing motion corrected cine imaging. J Cardiovasc Magn Reson 18:10
Merlocco A, Olivieri L, Kellman P et al (2018) Improved workflow for quantification of right ventricular volumes using free-breathing motion corrected cine imaging. Pediatr Cardiol 40:79–88
Piehler KM, Wong TC, Puntil KS et al (2013) Free-breathing, motion-corrected late gadolinium enhancement is robust and extends risk stratification to vulnerable patients. Circ Cardiovasc Imaging 6:423–432
Olivieri L, Cross R, O’Brien KJ et al (2016) Free-breathing motion-corrected late-gadolinium-enhancement imaging improves image quality in children. Pediatr Radiol 46:983–990
Hansen MS, Sørensen TS (2013) Gadgetron: an open source framework for medical image reconstruction. Magn Reson Med 69:1768–1776
Xue H, Inati S, Sorensen TS et al (2015) Distributed MRI reconstruction using gadgetron-based cloud computing. Magn Reson Med 73:1015–1025
Morray JP, Geiduschek JM, Ramamoorthy C et al (2000) Anesthesia-related cardiac arrest in children: initial findings of the pediatric perioperative cardiac arrest (POCA) registry. Anesthesiology 93:6–14
Ramamoorthy C, Haberkern CM, Bhananker SM et al (2010) Anesthesia-related cardiac arrest in children with heart disease: data from the pediatric perioperative cardiac arrest (POCA) registry. Anesth Analg 110:1376–1382
Malviya S, Voepel-Lewis T, Eldevik OP et al (2000) Sedation and general anaesthesia in children undergoing MRI and CT: adverse events and outcomes. Br J Anaesth 84:743–748
Serafini G, Zadra N (2008) Anaesthesia for MRI in the paediatric patient. Curr Opin Anaesthesiol 21:499–503
Kalkman CJ, Peelen L, Moons KG et al (2009) Behavior and development in children and age at the time of first anesthetic exposure. Anesthesiology 110:805–812
Schiller RM, Allegaert K, Hunfeld M et al (2018) Analgesics and sedatives in critically ill newborns and infants: the impact on long-term neurodevelopment. J Clin Pharmacol 58:S140–S150
Vanderby SA, Babyn PS, Carter MW et al (2010) Effect of anesthesia and sedation on pediatric MR imaging patient flow. Radiology 256:229–237
Jaimes C, Gee MS (2016) Strategies to minimize sedation in pediatric body magnetic resonance imaging. Pediatr Radiol 46:916–927
Dong SZ, Zhu M, Bulas D (2019) Techniques for minimizing sedation in pediatric MRI. J Magn Reson Imaging 50:1047–1054
Windram J, Grosse-Wortmann L, Shariat M et al (2012) Cardiovascular MRI without sedation or general anesthesia using a feed-and-sleep technique in neonates and infants. Pediatr Radiol 42:183–187
Shariat M, Mertens L, Seed M et al (2015) Utility of feed-and-sleep cardiovascular magnetic resonance in young infants with complex cardiovascular disease. Pediatr Cardiol 36:809–812
Cravero JP, Havidich JE (2011) Pediatric sedation - evolution and revolution. Paediatr Anaesth 21:800–809
Acknowledgments
This research was supported by the Intramural Research Program of the National Institutes of Health, National Heart, Lung, and Blood Institute.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Christopher, A.B., Quinn, R.E., Zoulfagharian, S. et al. Motion-corrected cardiac MRI is associated with decreased anesthesia exposure in children. Pediatr Radiol 50, 1709–1716 (2020). https://doi.org/10.1007/s00247-020-04766-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-020-04766-2