
Abstract
Background
Cine MRI has become a useful tool in the evaluation of patients with persistent obstructive sleep apnea (OSA) despite previous surgical intervention and in patients with underlying conditions that render them susceptible to multilevel airway obstruction. Findings on cine MRI studies have also increased our understanding of the mechanisms and anatomic causes of OSA in children.
Objective
To compare lingual tonsil size between children with OSA and a group of normal controls. In addition, a subanalysis was made of the group of children with OSA comparing lingual tonsils between children with and without underlying Down syndrome.
Materials and methods
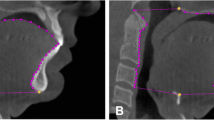
Children with persistent OSA despite previous palatine tonsillectomy and adenoidectomy and controls without OSA underwent MR imaging with sagittal fast spin echo inversion-recovery images, and lingual tonsils were categorized as nonperceptible at imaging or present and measurable. When present, lingual tonsils were measured in the maximum anterior-posterior diameter. If lingual tonsils were greater than 10 mm in diameter and abutting both the posterior border of the tongue and the posterior pharyngeal wall, they were considered markedly enlarged.
Results
There were statistically significant differences between the OSA and control groups for the presence vs. nonvisualization of lingual tonsils (OSA 33% vs. control 0%, P=0.0001) and mean diameter of the lingual tonsils (OSA 9.50 mm vs. control 0.0 mm, P=0.00001). Within the OSA group, there were statistically significant differences between children with and without Down syndrome for the three lingual tonsil width categories (P=0.0070) and occurrence of markedly enlarged lingual tonsils (with Down syndrome 35% vs. without Down syndrome 3%, P=0.0035).
Conclusions
Enlargement of the lingual tonsils is relatively common in children with persistent obstructive sleep apnea after palatine tonsillectomy and adenoidectomy. This is particularly true in patients with Down syndrome.



Similar content being viewed by others


References
Donnelly LF (2005) How I do it. OSA in pediatric patients: evaluation with cine MR sleep studies. Radiology 236:768–778
Gibson SE, Myer CM III, Strife JL, et al (1996) Sleep fluoroscopy for localization of upper airway obstruction in children. Ann Otol Rhinol Laryngol 105:678–683
Shott SR, Donnelly LF (2004) Cine magnetic resonance imaging: evaluation of persistent airway obstruction after tonsil and adenoidectomy in children with Down syndrome. Laryngoscope 114:1724–1729
Donnelly LF, Strife JL, Myer CM III (2001) Is sedation safe during dynamic sleep fluoroscopy of children with OSA? AJR 177:1031–1034
Fricke BL, Donnelly LF, Samuels PJ (2005) Is propofol anesthesia with unprotected airway safe for MRI cine evaluation of children with OSA? Pediatr Radiol 35:S69
Donnelly LF, Shott SR, LaRose CR, et al (2004) Causes of persistent OSA despite previous tonsillectomy and adenoidectomy in children with trisomy 21 as depicted on MR cine studies. AJR 183:175–181
Phillips DE, Rogers JH (1988) Down’s syndrome with lingual tonsil hypertrophy producing sleep apnea. J Laryngol Otol 102:1054–1055
Elia JC (1959) Lingual tonsillitis. Ann N Y Acad Sci 82:52–56
Dundar A, Ozunlu A, Sahan M, et al (1996) Lingual tonsil hypertrophy producing OSA. Laryngoscope 106(9 Pt 1):1167–1169
Guarisco JL, Littlewood SC, Butcher RB III (1990) Severe upper airway obstruction in children secondary to lingual tonsil hypertrophy. Ann Otol Rhinol Laryngol 99:621–624
Conache ID, Meikle D, O’Brien C (2002) Tracheostomy, lingular tonsillectomy and sleep-related breathing disorders. Br J Anaesth 88:724–726
American Thoracic Society (1996) Standards and indications for cardiopulmonary sleep studies in children. Am J Respir Crit Care Med 153:866–878
Donnelly LF, Surdulescu V, Chini BA, et al (2003) Upper airway motion depicted at cine MR imaging performed during sleep: comparison between young patients with and those without OSA. Radiology 227:239–245
Donnelly LF, Casper KA, Chen B, et al (2002) Defining normal upper airway motion in asymptomatic children during sleep by means of cine MR techniques. Radiology 223:176–180
Donnelly LF, Casper KA, Chen B (2002) Correlation on cine MR imaging of size of adenoid and palatine tonsils with degree of upper airway motion in asymptomatic sedated children. AJR 179:503–508
Abbott MB, Dardzinski BJ, Donnelly LF (2003) Using volume segmentation of cine MR data to evaluate dynamic motion of the airway in pediatric patients. AJR 181:857–859
Suto Y, Masuda E, Inoue Y, et al (1996) Sleep apnea syndrome: comparison of MR imaging of the oropharynx with physiologic indexes. Radiology 201:393–398
Suto Y, Matsuo T, Kato T, et al (1993) Evaluation of the pharyngeal airway in patients with sleep apnea: value of ultrafast MR imaging. AJR 160:311–314
Uong EC, McDonough JM, Tayag-Kier CE, et al (2001) Magnetic resonance imaging of the upper airway in children with Down syndrome. Am J Respir Crit Care Med 163:731–736
Marcus CL, Keens TG, Bautista DB, et al (1991) OSA in children with Down syndrome. Pediatrics 88:132–139
Southall DP, Stebbens VA, Mirza R, et al (1987) Upper airway obstruction with hypoxemia and sleep disruption in Down syndrome. Dev Med Child Neurol 29:734–742
Stebbens VA, Dennis J, Samuels MP, et al (1991) Sleep-related upper airway obstruction in a cohort with Down syndrome. Arch Dis Child 66:1333–1338
Kavanaugh KT, Kahane JC, Kardon B (1986) Risks and benefits of adenotonsillectomy for children with Down syndrome. Am J Mental Dis 91:22–29
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fricke, B.L., Donnelly, L.F., Shott, S.R. et al. Comparison of lingual tonsil size as depicted on MR imaging between children with obstructive sleep apnea despite previous tonsillectomy and adenoidectomy and normal controls. Pediatr Radiol 36, 518–523 (2006). https://doi.org/10.1007/s00247-006-0149-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-006-0149-7