
Abstract
Purpose
Colistin, which had not been used widely because of nephrotoxicity and neurotoxicity, has gained clinical importance in recent times due to the resurgence of multidrug-resistant Gram-negative bacilli. Very few studies, especially pharmacokinetic studies, have been performed with intravenous colistimethate sodium, and none in India. The aim of our study was to study the single-dose and steady-state pharmacokinetics of colistin in patients with multidrug-resistant Gram-negative bacilli infections.
Method
This was a prospective open-label pharmacokinetic study done in an intensive care unit in a tertiary care hospital on 15 critically ill patients with proven multidrug-resistant Gram-negative bacilli infection. Colistimethate sodium was injected as intermittent intravenous infusions in accordance with the recommendations on the package insert. For patients weighing ≥60 kg with a normal renal function or with a creatinine clearance (CLCR) of between 20 and 50 ml/min, the drug was administered at 2 million international units (MIU) every 8 h; for those with a CLCR of 10–20 ml/min, the dose was 2 MIU every 12 h. Those patients who weighed <60 kg were administered 50,000 IU/kg/day in three divided doses at 8-h intervals. Both single-dose and steady-state pharmacokinetics of colistin were determined and correlated with clinical outcomes.
Results
A wide inter-individual variation was observed in pharmacokinetic parameters. The median (range) of the maximum plasma drug concentration/minimum inhibitory concentration (Cmax/MIC) ratio for Acinetobacter spp. was 13.4 (1.3–40.3) following the administration of a single dose of colistimethate sodium and 26.3 (0.9–64.9) at steady-state. For Pseudomonas spp., these values were 3.18 (1.6–23.1) following the single dose and 3.82 (2.3–10.9) at steady-state. For those patients whose cultures grew Acinetobacter spp., an optimum value of the Cmax/MIC ratio of >8 was achieved in seven of nine patients after the single dose and in seven of eight patients at steady-state. For those patients whose cultures grew Pseudomonas spp, only one patient after the single dose and one patient at steady-state achieved a Cmax/MIC ratio of >8. A significant association was noted between dose and survival, and a trend was observed with patients weighing ≤60 kg (who received 50,000 IU/kg/day instead of 6 MIU/day for those >60 kg) having an increased mortality.
Conclusion
The pharmacokinetic parameters of colistin were comparable to those reported in previous studies in critically ill patients. However, the recommended dose may be inadequate to maintain the Cmax/MIC ratio to an optimal level—at least in patients infected with Pseudomonas spp. The dose recommendation should be based only on creatinine clearance and not body weight.
Similar content being viewed by others


Introduction
The escalating incidence of infections due to multidrug resistant (MDR) Gram-negative bacilli, particularly among critically ill patients, is a worldwide problem and is associated with significant morbidity and mortality [1–3]. In the search for effective antimicrobials, there has been an increased interest in an old antibiotic, colistin [4–7]. Although introduced in 1959, the drug has not been widely used because of its association with a high incidence of nephrotoxicity and neurotoxicity [8].
Colistin is a cationic, multicomponent (including colistin A and B) lipopeptide antibiotic that is intravenously administered as its prodrug, colistimethate sodium [9]. The drug exhibits concentration-dependent bactericidal activity against Acinetobacter baumannii [10] and Pseudomonas aeruginosa [11], and several studies have shown its efficacy in the treatment of the infections caused by these microorganisms [12–14]. The European Committee on Antimicrobial Susceptibility Testing has specified a minimum inhibitory concentration (MIC) of ≤2 mg/l for these microorganisms to be called susceptible [15].
There is a dearth of pharmacological information on colistin, possibly because it did not undergo rigorous drug development studies prior to marketing as is required today. The recent interest in colistin has highlighted the lack of adequate pharmacokinetic and pharmacodynamic data to guide dosing [7, 16]. Very few studies have been conducted to evaluate the pharmacokinetics of colistin following intravenous colistimethate sodium worldwide [17–21], and none have been conducted in India. Therefore, the aim of our study was to assess the single-dose as well as steady-state pharmacokinetics of the colistin base in critically ill patients with MDR Gram-negative infections in a tertiary care hospital in India.
Patients and methods
This was a prospective, non-comparative, open label study conducted between September 2009 and August 2010. Institutional Review Board (IRB) approval was obtained, and the study was registered with Clinical Trial Registry of India (CTRI/2009/091/000252).
Patients
Critically ill patients (14 adults, 1 adolescent) admitted to the medical intensive care unit with bacteriologically documented MDR Gram-negative infections were enrolled in the study after written informed consent had been obtained from the patients or their legally accepted representatives. MDR infections due to Gram-negative bacilli were defined as resistance to three or more of the antimicrobials, including penicillins, cephalosporins, betalactams + beta lactamase inhibitors, fluoroquinolones, carbapenems, but sensitivity to colistin as per microbiological culture report [22]. Detailed history and physical examination findings were noted daily, and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores and findings from chest X-ray, 12-lead electrocardiogram and routine hematological and biochemical investigations were recorded at baseline. The baseline creatinine clearance (CLCR) (estimated by Cockcroft–Gault formula [23]) guided the calculation of dose, and the measurement was repeated daily. A urine pregnancy test was performed in women of child bearing age before the administration of colistimethate sodium. Blood and bronchoalveolar lavage specimens were obtained prior to drug administration and processed for Gram stain and culture, antibiotic sensitivity and a measurement of the MIC for colistin. Patients with a CLCR of <10 ml/min, aged <18 years (one adolescent of age 15 years was included after obtaining permission from the IRB) or >65 years and/or diagnosed as myasthenia gravis were excluded; pregnant and breastfeeding women were also excluded.
The patients were administered the drug as described below for a duration ranging from a minimum of 8 to a maximum of 14 days depending on clinical need. Only those patients who received the drug for at least 8 days were considered to have completed the study. If the patients’ CLCR fell to <10 ml/min during the treatment, they were withdrawn from the study.
Outcomes
Clinical outcomes
Clinical cure was defined when the complete resolution of clinical findings (signs and symptoms, leukocytosis and chest X-ray) were noted. If there was partial resolution, it was considered as clinical improvement. Clinical failure was defined as the persistence or worsening of symptoms and/or signs of infection at 72 h after starting colistimethate sodium.
Bacteriological outcomes
The outcome was labeled eradication when there was no growth of the pathogen in the final culture (last day of colistimethate sodium injection), and persistence if the growth was seen regardless of clinical outcome. When microbiological assessment was not possible, it was considered as undetermined.
Safety outcomes
The safety parameters that were included in the study were mortality, adverse events and any clinically significant changes in the laboratory values.
Methods
Drug administration
All patients received colistimethate sodium (XylistinTM; Batch number XP-9001; Cipla Ltd., Mumbai Central, Mumbai, India) administered intravenously over 30 min at a dose calculated according to the recommendations on the product’s label. For patients weighing ≥60 kg with normal renal function or with a CLCR between 20 and 50 ml/min, the drug was administered at 2 million international units (MIU) every 8 h; for those with a CLCR of 10–20 ml/min, 2 MIU was administered every 12 h. Patients weighing <60 kg were administered 50,000 IU/kg/day in three divided doses at 8-h intervals. The powder was dissolved in 50 ml normal saline for infusion.
Blood sampling
Blood samples (3 ml in a plain test tube) were collected on day 1 (single dose) and day 4 (steady-state) following the initiation of colistimethate sodium injections, prior to dose administration and at 30 and 40 min and 1, 2, 4, 6 and 8 h post-drug administration. Pre-dose samples were also collected on days 2, 3, 5, 6 and 7. The serum was separated and stored at −70 °C pending analysis.
Drug estimation by liquid chromatography–tandem mass spectrometry
A bioanalytical method for the simultaneous assay of both colistin A and colistin B from serum samples was developed and validated based on an earlier method described by Zheng Ma et al. [24]. Analytes (colistin A and B) were extracted from serum samples by protein precipitation followed by solid phase extraction. Quantitation was performed using the liquid chromatography–tandem mass spectrometry instrument API 4000 (Applied Biosystems, Foster City, CA) by multiple reaction monitoring transitions as 585.60 → 101.20 and 578.60 → 227.60 for colistin A and colistin B, respectively. Polymyxin B was used as an internal standard. The chromatographic method involved the use of volatile ion pairing reagent heptaflurobutyric acid as mobile phase additive and a C18 analytical column. The use of an ion pairing reagent helped in achieving good sensitivity, resolution of analytes from endogenous matrix and good peak shapes. The drug concentration curve was linear in serum samples between 9.6 and 1434.5 ng/ml for colistin A and between 30.0 and 4493.8 ng/ml for colistin B. The matrix effect was evaluated using the results from post-column infusion and post-extraction addition experiments. This method was validated for specificity, selectivity, sensitivity, precision and accuracy, stability (stock solution, post-preparative, short term, freeze-thaw and long term), recovery, dilution integrity, re-injection reproducibility and ruggedness. The precision for colistin A and colistin B ranged between 2.28 and 9.05 % and between 2.82 and 6.34 %, respectively. The accuracy for colistin A and colistin B ranged between 93.75 and 105.23 % and between 96.53 and 106.91 %, respectively.
Statistical analysis
No formal sample size calculations were performed. The pharmacokinetic analysis was performed using WinNonLin ver. 5.3; Pharsight, St. Louis, MO). In each participant, age, weight, APACHE II score, colistin dose, CLCR and all pharmacokinetic parameters were considered as quantitative continuous variables and expressed as the median (range). All significant associations were represented with the 95 % confidence interval (CI). Sex and survival were considered as categorical variables. The normality of the data was checked by using the Kolmogorov–Smirnov test.
Post hoc analysis
Although the study was primarily envisaged as a pharmacokinetic study, as the study was progressing, we observed certain differences in the clinical outcomes between patients who had received the drug at different doses. Also, there is a paucity of data on survival with colistin. Hence, a number of post hoc tests were carried out. The Spearman rank correlation coefficient was calculated using single-dose and steady-state maximum plasma drug concentration (Cmax) as dependant variables and age, APACHE II score, CLCR and dose of colistimethate sodium as independent variables. To assess the correlation between the single-dose and steady-state Cmax/MIC ratio, the Spearman rank correlation test was used with the APACHE II score and dose of colistimethate sodium as independent variables. A binary logistic regression analysis was carried out between various predictor variables (age, body weight, APACHE II scores, CLCR, dosage, single-dose and steady-state Cmax) and survival using Minitab ver. 16.0 statistical software (2010; Minitab Inc., State College, PA: www.minitab.com), and correlation between the predictor variables with single-dose and steady-state Cmax and single-dose and steady-state Cmax/MIC ratio was performed using the Spearman rank correlation coefficient with GraphPad Instat ver. 3.05 for Windows 95 (GraphPad Software, San Diego CA: www.graphpad.com). A p value of <5 % was considered to be significant.
Results
Demographic data
Of the 15 patients enrolled, eight were men and seven were women. The median (range) APACHE II score was 9 (4–16) and median (range) CLCR was 125 (49.16–220.8) ml/min. The indication for administering colistimethate sodium was ventilator-associated pneumonia in all of the study patients. Demographic details of the individual study patients are described in Table 1. Of the 15 patients, four died before completing the study, seven showed clinical cure and four showed clinical improvement. Of the latter, one patient died due to progression of the underlying pathology.
Bacteriological profile and outcome
The bacteriological profile is shown in Table 1. A total of 13 samples showed resistance to imipenem. The MICs for these organisms were available for 12 patients and the median (range) were 0.38 (0.25–2) and 1.5 (1–2) μg/ml for Acinetobacter spp. and Pseudomonas spp., respectively. The details of bacteriological and other outcomes are given in Table 2.
Dose of colistimethate sodium
Of the 15 patients, 11 received 2 MIU colistimethate sodium at 8-h intervals while four received 50,000 IU/kg/day in three divided doses calculated on the basis of body weight and CLCR. The median (range) dose of colistimethate sodium was 6 (2.5–6) MIU per day.
Pharmacokinetic parameters
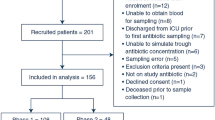
Single-dose pharmacokinetic data were available for 13 patients (data could not be obtained in 2 patients due to analytical problems), and both the single-dose and steady-state pharmacokinetic data were available for 11 patients (2 of 13 patients died within day 4 of colistin treatment initiation).
A wide inter-individual variability was seen in the pharmacokinetic parameters. The median (range) Cmax, elimination half life (t½) and clearance (CL) were 4.6 (2.5–23.2) μg/ml, 2.7 (1.1–4.6) h and 1.3 (1.0–2.1) ml/min/kg, respectively, after a single dose, and 5.4 (1.8–21.8) μg/ml, 3.3 (1.2–5.4) h and 1.1 (0.7–1.9) ml/min/kg, respectively, at steady-state (after day 4 dose). The summary of the various pharmacokinetic parameters is depicted in Table 3, and mean concentrations following the single dose and at steady-state at various time points are shown in Figs. 1 and 2, respectively.

Single-dose time-concentration plot of colistin (n = 13). Data are presented as the mean and standard deviation (SD; whiskers)

Steady-state time-concentration plot of colistin (n = 11). Data are presented as the mean and SD (whiskers)
The median (range) Cmax/MIC ratio following a single dose and at steady-state was 13.4 (1.3–40.3) and 26.3 (0.9–64.9), respectively, for Acinetobacter spp. and 3.2 (1.6–23.1) and 3.8 (2.3–10.9), respectively, for Pseudomonas spp..
Other analyses
Binary logistic regression showed a significant association of survival with the dosage of the drug (p = 0.046). Three of the four patients weighing ≤60 kg (received 50,000 IU/kg/day) died and two of the 11 weighing >60 kg (received 2 M IU at 8-h intervals) died (Fisher exact probability test p = 0.077). The dose of colistimethate sodium was significantly correlated with Cmax (single-dose: ρ = 0.65, 95 % CI 0.14–0.89, p = 0.02; steady-state: ρ = 0.78, 95 % CI 0.33–0.94, p = 0.01) and Cmax/MIC ratio (single-dose: ρ = 0.57, 95 % CI 0.01–0.85, p = 0.04; steady-state: ρ = 0.65, 95 % CI 0.09–0.89, p = 0.02). A significant correlation was also found between steady-state Cmax and body weight (ρ = 0.66, 95 % CI 0.07–0.90, p = 0.03).
Adverse events
Adverse events noted in the study participants are mentioned in Table 2. Amongst those with elevated liver enzymes, only one had a possible causal relation to the drug. Hyponatremia, hypokalemia and convulsion were seen in one participant (possibly related) and a serious adverse event in the form of death due to septicemia was reported in five patients (causality: unlikely). No other major adverse events were noted.
Concomitant medications
Broadly, the drug classes that were administered concomitantly included other antimicrobials, corticosteroids, biologicals, anti-coagulants, anticonvulsants, intravenous fluids and cardiac inotropes. None of these are known to interact with colistimethate sodium pharmacokinetically.
Discussion
Our study is the first to be carried out in India that documents the single-dose and steady-state pharmacokinetics of colistin in critically ill patients. The pharmacokinetic parameters showed wide inter-individual variability, and the single-dose and steady-state pharmacokinetic parameters did not differ significantly. The steady-state parameters were similar to those reported in critically ill Caucasian patients [18, 20], and the overall survival rate of 66.67 % was also comparable to that reported in other studies [25, 26].
The single-dose and steady-state Cmax [median (range): 4.6 (2.5–23.1) vs. 5.4 (1.8–21.8) μg/ml, respectively] in our study were lower than those reported in patients with cystic fibrosis [ 21.4 (5) vs. 23 (8) mg/l, respectively) [21]. One possible explanation is the higher volume of distribution seen in critically ill patients [27]. The volume of distribution in the patients included in our study [median (range)] was 0.3 (0.2–0.5) after both the single dose and at steady-state as compared to cystic fibrosis patients [0.09 (0.02) vs. 0.09 (0.03) l/kg, respectively) [21].
Colistin exhibits concentration-dependant bactericidal activity against Pseudomonas aeruginosa and Acinetobacter baumannii [11, 28]. However, there is no consensus on the optimal Cmax/MIC ratio for colistin [18], whereas for the other concentration-dependent bactericidal antibiotics, an optimal Cmax/MIC ratio of 8–10 is recommended [29, 30]. The median (range) Cmax/MIC value in our study following the single dose and at steady-state was 13.4 (1.3–40.3) and 26.3 (0.9–64.9), respectively, for Acinetobacter spp. and 3.2 (1.6–23.1) and 3.8 (2.3–10.9), respectively, for Pseudomonas spp.. Among those patients whose cultures grew Acinetobacter spp., MIC and Cmax values were available for nine patients following the single dose and for eight patients at steady-state. Of these, seven each had a Cmax/MIC ratio of >8. Of the four patients whose cultures grew Pseudomonas spp., one each had a Cmax/MIC ratio of >8 after the single dose and at steady-state, indicating that higher dosing may be required for patients with Pseudomonas spp. infection.
The dose and dosing frequency of colistimethate sodium was determined in this study taking into consideration body weight and CLCR (as per the product insert). None of our patients had a CLCR of <20 ml/min, and therefore the dosing was primarily based on weight. The four patients who weighed ≤60 kg received a considerably smaller dose of colistimethate sodium (2.5 M IU/day and 2.75 M IU/day in two patients each) and three of the four succumbed. In contrast, nine of the 11who weighed >60 kg and received 6 MIU/day survived, indicating that adequate dosing is necessary for best results. It is important to note that among the many factors that were tested for their association with survival in our study, only the dose of the drug was found to be significantly associated. The Cmax/MIC ratios obtained in our study for both the organisms reiterate this observation. One of the major reasons for colistin going into disrepute was safety concerns. Our study indicates that the use of doses up to 6 MIU/day is safe even in critically ill patients, thereby corroborating the findings from recent reviews by Florescu et al. [26] and Couet et al [31]. Other authors have reported the safe use of colistimethate sodium even at doses of 9 MIU per day [32] and with a loading dose of 6 MIU [33]. It would appear relevant to suggest changes to the label so that dosing is based on CLCR only and not also on body weight.
The main limitations of our study are that (1) we did not measure urinary concentrations of colistin and therefore could not determine renal clearance, (2) the multivariate analysis is limited by the fact that the baseline diagnosis which itself influences prognosis is not taken for consideration due to small sample size and (3) the survival analysis was carried out following completion of the study.
Conclusion
Among the patients enrolled in our study, colistin was well tolerated, and no events of either renal toxicity or neurotoxicity were noted at the dose administered. Cmax was found to be comparable to that of previous studies but appears to be inadequate to maintain the Cmax/MIC ratio to an optimal level—at least for Pseudomonas spp. Dose revision may need to be considered for patients weighing ≤60 kg. Overall, the pharmacokinetic–pharmacodynamic information obtained from this study may be a useful tool in antibiotic selection and implies therapeutic benefits of colistin in hospital-acquired MDR Gram-negative bacilli infections.
References
D’Agata EMC (2004) Rapidly rising prevalence of nosocomial multidrug resistant, Gram negative bacilli: a 9 year surveillance study. Infect Control Hosp Epidemiol 25:842–846
Doughlas MW, Mulholland K, Denyer V et al (2001) Multidrug resistant Pseudomonas aeruginosa outbreak in a burns unit—an infection control study. Burns 7:131–135
Livermore DM (2002) Multiple mechanisms of antimicrobial resistance in Pseudomonas aeruginosa: or worst nightmare? Clin Infect Dis 34:634–640
Li J, Nation RI, Milne RW, Turnidge JD et al (2005) Evaluation of colistin as an agent against multi-resistant gram-negative bacteria. Int J Antimicrob Agents 25:11–25
Livermore DM (2004) The need for new antibiotics. Clin Microbiol Infect 10(4):1–9
Li J, Nation RL, Turpidge JD et al (2006) Colistin: the re-emerging antibiotic for multidrug-resistant Gram-negative bacterial infections. Lancet Infect Dis 6:589–601
Landman D, Georgescu C, Martin DA et al (2008) Polymyxins revisited. Clin Microbiol Rev 21:449–465
Durakovic N, Radojcic V, Boban A et al (2011) Efficacy and safety of colistin in the treatment of infections caused by multi-drug resistant Pseudomonas aeruginosa in patients with hematologic malignancy: a matched pair analysis. Intern Med 50:1009–1013
Orwa JA, Govaerts R, Busson R et al (2001) Isolation and structural characterization of colistin components. J Antibiot (Tokyo) 54:595–599
Owen RJ, Li J, Nation RL et al (2007) In vitro pharmacodynamics of colistin against Acinetobacter baumannii clinical isolates. J Antimicrob Chemother 59:473–477
Li J, Turnidge J, Milne R et al (2001) In vitro pharmacodynamic properties of colistin and colistin methanesulfonate against Pseudomonas aeruginosa isolates from patients with cystic fibrosis. Antimicrob Agents Chemother 45:781–785
Koomanachai P, Tiengrim S, Kiratisin et al (2007) Efficacy and safety of colistin (colistimethate sodium) for therapy of infections caused by multidrug resistant Pseudomonas aeruginosa and Acinetobacter baumannii in Siriraj hospital, Bangkok, Thailand. Int J Infect Dis 11:402–406
Pintado V, Miguel LGS, Grill F et al (2008) Intravenous colistin sulphomethate sodium for therapy of infections due to multidrug-resistant Gram-negative bacteria. J Infect 56:185–190
Hachem RY, Chemaly RF, Ahmar CA et al (2007) Colistin is effective in treatment of infections caused by multidrug-resistant Pseudomonas aeruginosa in cancer subjects. Antimicrob Agents Chemother 51:1905–1911
European Committee on Antimicrobial Susceptibility Testing. Miscellaneous antimicrobials—EUCAST clinical MIC breakpoints 2009-12-13 (v 2.3). Available at: www.srga.org/eucastwt/MICTAB/MICmiscellaneous.html. Accessed 2 Feb 2012
Nation RL, Li J (2007) Optimizing use of colistin and polymyxin B in the critically ill. Semin Respir Crit Care Med 28:604–614
Li J, Coulthard K, Milne R et al (2003) Steady-state pharmacokinetics of intravenous colistin methanesulphonate in patients with cystic fibrosis. J Antimicrob Chemother 52:987–992
Markou N, Markantonis SL, Dimitrakis E et al (2008) Colistin serum concentrations after intravenous administration in critically ill patients with serious multidrug resistant, Gram negative bacilli infections: a prospective, open label, uncontrolled study. Clin Ther 30:143–151
Ratjen F, Rietschel E, Kasel D et al (2006) Pharmacokinetics of inhaled colistin in patients with cystic fibrosis. J Antimicrob Chemother 57:306–311
Imberti R, Cusato M, Villani P et al (2010) Steady-state pharmacokinetics and bronchoalveolar lavage concentration of colistin in critically ill patients after intravenous colistin methanesulphonate administration. Chest 138:1333–1339
Reed MD, Stern RC, O’Riordan MA et al (2001) The pharmacokinetics of colistin in patients with cystic fibrosis. J Clin Pharmacol 41:645–654
Giske CG, Monnet DL, Cars O et al (2008) Clinical and economic impact of common multidrug-resistant Gram negative bacilli. Antimicrob Agents Chemother 52:813–821
National Kidney Foundation Kidney Disease Outcomes Quality Initiative. KDOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Available at: http://www.kidney.org/professionals/kdoqi/guidelines_ckd/p4_class_g1.htm. Accessed 26 Nov 2012
Ma Z, Wang J, Gerber JP et al (2008) Determination of colistin in human plasma, urine and other biological samples using LC-MS/MS. J Chromatogr B 862:205–212
Sabuda DM, Laupland K, Pitout J et al (2008) Utilization of colistin for treatment of multidrug-resistant Pseudomonas aeruginosa. Can J Infect Dis Med Microbiol 19:413–418
Florescu DF, Qiu F, McCartan MA et al (2012) What is the efficacy and safety of colistin for the treatment of ventilator-associated pneumonia? A systematic review and meta-regression. Clin Infect Dis 54:670–680
Mehrotra R, Gaudie RD, Palazzo M (2004) Antibiotic pharmacokinetic and pharmacodynamic considerations in critical illness. Intensive Care Med 30:2145–2156
Li J, Rayner CR, Nation RL et al (2006) Heteroresistance to colistin in multidrug-resistant Acinetobacter baumannii. Antimicrob Agents Chemother 50:2946–2950
De Gaudio AR, Rinaldi S, Adembri C (2012) Systemic antibiotics. In: Van Saene HKF, Silvestri L, Del la Cal MA, Gullo A (eds) Infection control in the intensive care unit. Springer SBM, Milan, p 73
Levison ME (2004) Pharmacodynamics of antimicrobial drugs. Infect Dis Clin North Am 18:451–465
Couet W, Gregoire N, Marchand S et al (2012) Colistin pharmacokinetics: the fog is lifting. Clin Microbiol Infect 18:30–39
Plachouras D, Karvanen M, Friberg LE et al (2009) Population pharmacokinetic analysis of colistin methanesulfonate and colistin after intravenous administration in critically ill patients with infections caused by gram negative bacteria. Antimicrob Agents Chemother 53:3430–3436
Mohamed AF, Karaiskos I, Plachouras D et al (2012) Application of a loading dose of colistin methanesulfonate in critically ill patients: population pharmacokinetics, protein binding, and prediction of bacterial kill. Antimicrob Agents Chemother 56:4241–4249
Acknowledgments
We thank Dr. Sanjay Oak, Director for permission to use institutional facilities to conduct the study, Dr. Syedunissa Khan for rendering help in data collection and Mr. Krishnan Iyer from Sitec Lab for assistance in drug assay.
Conflict of interest
SPJ, RDN and JAG are employees of Cipla pharmaceuticals Ltd. RKN is an employee of Sitec Labs (Pvt.) Ltd.
Financial support
This study was sponsored by Cipla Ltd.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karnik, N.D., Sridharan, K., Jadhav, S.P. et al. Pharmacokinetics of colistin in critically ill patients with multidrug-resistant Gram-negative bacilli infection. Eur J Clin Pharmacol 69, 1429–1436 (2013). https://doi.org/10.1007/s00228-013-1493-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-013-1493-9