
Abstract
Summary
While type 2 diabetes (T2D) is associated with higher skeletal fragility, specific risk stratification remains incompletely understood. We found volumetric bone mineral density, geometry, and serum sclerostin differences between low-fracture risk and high-fracture risk T2D women. These features might help identify T2D individuals at high fracture risk in the future.
Introduction
Diabetic bone disease, an increasingly recognized complication of type 2 diabetes mellitus (T2D), is associated with high skeletal fragility. Exactly which T2D individuals are at higher risk for fracture, however, remains incompletely understood. Here, we analyzed volumetric bone mineral density (vBMD), geometry, and serum sclerostin levels in two specific T2D subsets with different fracture risk profiles. We examined a T2D group with prior history of fragility fractures (DMFx, assigned high-risk group) and a fracture-free T2D group (DM, assigned low-risk group) and compared their results to nondiabetic controls with (Fx) and without fragility fractures (Co).
Methods
Eighty postmenopausal women (n = 20 per group) underwent quantitative computed tomography (QCT) to compute vBMD and bone geometry of the proximal femur. Additionally, serum sclerostin, vitamin D, parathyroid hormone (PTH), HbA1c, and glomerular filtration rate (GFR) levels were measured. Statistical analyses employed linear regression models.
Results
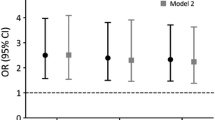
DMFx subjects exhibited up to 33 % lower femoral neck vBMD than DM subjects across all femoral sites (−19 % ≤ ΔvBMD ≤ −33 %, 0.008 ≤ p ≤0.021). Additionally, DMFx subjects showed significantly thinner cortices (−6 %, p = 0.046) and a trend toward larger bone volume (+10 %, p = 0.055) relative to DM women and higher serum sclerostin levels when compared to DM (+31.4 %, p = 0.013), Fx (+25.2 %, p = 0.033), and control (+22.4 %, p = 0.028) subjects.
Conclusion
Our data suggest that volumetric bone parameters by QCT and serum sclerostin levels can identify T2D individuals at high risk of fracture and might therefore show promise as clinical tools for fracture risk assessment in T2D. However, future research is needed to establish diabetes-specific QCT- and sclerostin-reference databases.

Similar content being viewed by others

References
Whiting DR, Guariguata L, Weil C, Shaw J (2011) IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract 94:311–321
Brownlee M (2005) The pathobiology of diabetic complications: a unifying mechanism. Diabetes 54:1615–1625
Schwartz AV, Sellmeyer DE, Ensrud KE, Cauley JA, Tabor HK, Schreiner PJ, Jamal SA, Black DM, Cummings SR (2001) Older women with diabetes have an increased risk of fracture: a prospective study. J Clin Endocrinol Metab 86:32–38
de Liefde I, van der Klift M, de Laet CE, van Daele PL, Hofman A, Pols HA (2005) Bone mineral density and fracture risk in type-2 diabetes mellitus: the Rotterdam Study. Osteoporos Int 16:1713–1720
Janghorbani M, Van Dam RM, Willett WC, Hu FB (2007) Systematic review of type 1 and type 2 diabetes mellitus and risk of fracture. Am J Epidemiol 166:495–505
Schwartz AV, Vittinghoff E, Bauer DC et al (2011) Association of BMD and FRAX score with risk of fracture in older adults with type 2 diabetes. JAMA 305:2184–2192
Giangregorio LM, Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis JA (2012) FRAX underestimates fracture risk in patients with diabetes. J Bone Miner Res 27:301–308
Patsch JM, Burghardt AJ, Yap SP, Baum T, Schwartz AV, Joseph GB, Link TM (2013) Increased cortical porosity in type 2 diabetic postmenopausal women with fragility fractures. J Bone Miner Res 28:313–324
Patsch JM, Li X, Baum T, Yap SP, Karampinos DC, Schwartz AV, Link TM (2013) Bone marrow fat composition as a novel imaging biomarker in postmenopausal women with prevalent fragility fractures. J Bone Miner Res 28:1721–1728
Riggs BL, Melton LJ, Robb RA, Camp JJ, Atkinson EJ, McDaniel L, Amin S, Rouleau PA, Khosla S (2008) A population-based assessment of rates of bone loss at multiple skeletal sites: evidence for substantial trabecular bone loss in young adult women and men. J Bone Miner Res 23:205–214
Melton LJ 3rd, Riggs BL, Leibson CL, Achenbach SJ, Camp JJ, Bouxsein ML, Atkinson EJ, Robb RA, Khosla S (2008) A bone structural basis for fracture risk in diabetes. J Clin Endocrinol Metab 93:4804–4809
Register TC, Hruska KA, Divers J et al (2014) Sclerostin is positively associated with bone mineral density in men and women and negatively associated with carotid calcified atherosclerotic plaque in men from the African American-Diabetes Heart Study. J Clin Endocrinol Metab 99:315–321
Yamamoto M, Yamauchi M, Sugimoto T (2013) Elevated sclerostin levels are associated with vertebral fractures in patients with type 2 diabetes mellitus. J Clin Endocrinol Metab 98:4030–4037
Ardawi MS, Akhbar DH, Alshaikh A, Ahmed MM, Qari MH, Rouzi AA, Ali AY, Abdulrafee AA, Saeda MY (2013) Increased serum sclerostin and decreased serum IGF-1 are associated with vertebral fractures among postmenopausal women with type-2 diabetes. Bone 56:355–362
Sarahrudi K, Thomas A, Albrecht C, Aharinejad S (2012) Strongly enhanced levels of sclerostin during human fracture healing. J Orthop Res 30:1549–1555
Genant HK, Wu CY, van Kuijk C, Nevitt MC (1993) Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 8:1137–1148
Lenchik L, Rogers LF, Delmas PD, Genant HK (2004) Diagnosis of osteoporotic vertebral fractures: importance of recognition and description by radiologists. AJR Am J Roentgenol 183:949–958
Voormolen MH, van Rooij WJ, van der Graaf Y, Lohle PN, Lampmann LE, Juttmann JR, Sluzewski M (2006) Bone marrow edema in osteoporotic vertebral compression fractures after percutaneous vertebroplasty and relation with clinical outcome. AJNR 27:983–988
Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J, Eknoyan G (2003) National kidney foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med 139:137–147
Miller WG (2009) Estimating glomerular filtration rate. Clin Chem Lab Med CCLM / FESCC 47:1017–1019
Fazeli PK, Ackerman KE, Pierce L, Guereca G, Bouxsein M, Misra M (2013) Sclerostin and Pref-1 have differential effects on bone mineral density and strength parameters in adolescent athletes compared with non-athletes. Osteoporos Int 24:2433–2440
Taylor JR (1997) An introduction to error analysis: the study of uncertainties in physical measurements. University Science Books, Sausalito
Lang T, LeBlanc A, Evans H, Lu Y, Genant H, Yu A (2004) Cortical and trabecular bone mineral loss from the spine and hip in long-duration spaceflight. J Bone Miner Res 19:1006–1012
Black DM, Bilezikian JP, Ensrud KE, Greenspan SL, Palermo L, Hue T, Lang TF, McGowan JA, Rosen CJ (2005) One year of alendronate after one year of parathyroid hormone (1-84) for osteoporosis. N Engl J Med 353:555–565
Cohen A, Lang TF, McMahon DJ et al (2012) Central QCT reveals lower volumetric BMD and stiffness in premenopausal women with idiopathic osteoporosis, regardless of fracture history. J Clin Endocrinol Metab 97:4244–4252
Black DM, Bouxsein ML, Marshall LM, Cummings SR, Lang TF, Cauley JA, Ensrud KE, Nielson CM, Orwoll ES, Osteoporotic Fractures in Men Research G (2008) Proximal femoral structure and the prediction of hip fracture in men: a large prospective study using QCT. J Bone Miner Res 23:1326–1333
Mirza FS, Padhi ID, Raisz LG, Lorenzo JA (2010) Serum sclerostin levels negatively correlate with parathyroid hormone levels and free estrogen index in postmenopausal women. J Clin Endocrinol Metab 95:1991–1997
Rejnmark L, Vestergaard P, Brot C, Mosekilde L (2011) Increased fracture risk in normocalcemic postmenopausal women with high parathyroid hormone levels: a 16-year follow-up study. Calcif Tissue Int 88:238–245
Thorson S, Prasad T, Sheu Y, Danielson ME, Arasu A, Cummings SR, Cauley JA (2013) Sclerostin and bone strength in women in their 10th decade of life. J Bone Miner Res 28:2008–2016
Strotmeyer ES, Cauley JA, Schwartz AV et al (2004) Diabetes is associated independently of body composition with BMD and bone volume in older white and black men and women: the health, aging, and body composition study. J Bone Miner Res 19:1084–1091
Leslie WD, Rubin MR, Schwartz AV, Kanis JA (2012) Type 2 diabetes and bone. J Bone Miner Res 27:2231–2237
Seeman E (2003) Periosteal bone formation—a neglected determinant of bone strength. N Engl J Med 349:320–323
Costa AG, Cusano NE, Silva BC, Cremers S, Bilezikian JP (2011) Cathepsin K: its skeletal actions and role as a therapeutic target in osteoporosis. Nat Rev 7:447–456
Kadoglou NP, Daskalopoulou SS, Perrea D, Liapis CD (2005) Matrix metalloproteinases and diabetic vascular complications. Angiology 56:173–189
Vashishth D (2014) Talk on effects of advanced glycation end products on bone ASBMR symposium “The effects of diabetes and disordered energy metabolism on skeletal health”
Garcia-Hernandez A, Arzate H, Gil-Chavarria I, Rojo R, Moreno-Fierros L (2012) High glucose concentrations alter the biomineralization process in human osteoblastic cells. Bone 50:276–288
Monnier VM, Kohn RR, Cerami A (1984) Accelerated age-related browning of human collagen in diabetes mellitus. Proc Natl Acad Sci U S A 81:583–587
Dallas SL, Prideaux M, Bonewald LF (2013) The osteocyte: an endocrine cell … and more. Endocr Rev 34:658–690
Botolin S, McCabe LR (2006) Chronic hyperglycemia modulates osteoblast gene expression through osmotic and non-osmotic pathways. J Cell Biochem 99:411–424
Wittrant Y, Gorin Y, Woodruff K, Horn D, Abboud HE, Mohan S, Abboud-Werner SL (2008) High d(+)glucose concentration inhibits RANKL-induced osteoclastogenesis. Bone 42:1122–1130
Liu C, Al-Dujaili H, Fischer C, Wang L, You L (2013) Altered osteocyte mechanosensitivity in response to elevated extracellular glucose levels. J Bone Miner Res 28 (Suppl 1) SU 0283, available at http://www.asbmr.org/education/AbstractDetail?aid=2bfbb710-d034-489e-b0af8a2b716c8861, Accessed November 29, 2013
Gaudio A, Pennisi P, Bratengeier C, Torrisi V, Lindner B, Mangiafico RA, Pulvirenti I, Hawa G, Tringali G, Fiore CE (2010) Increased sclerostin serum levels associated with bone formation and resorption markers in patients with immobilization-induced bone loss. J Clin Endocrinol Metab 95:2248–2253
Spatz JM, Fields EE, Yu EW, Divieti Pajevic P, Bouxsein ML, Sibonga JD, Zwart SR, Smith SM (2012) Serum sclerostin increases in healthy adult men during bed rest. J Clin Endocrinol Metab 97:E1736–E1740
Frassetto LA, Sebastian A (2012) How metabolic acidosis and oxidative stress alone and interacting may increase the risk of fracture in diabetic subjects. Med Hypotheses 79:189–192
Modder UI, Hoey KA, Amin S, McCready LK, Achenbach SJ, Riggs BL, Melton LJ 3rd, Khosla S (2011) Relation of age, gender, and bone mass to circulating sclerostin levels in women and men. J Bone Miner Res 26:373–379
Durosier C, van Lierop A, Ferrari S, Chevalley T, Papapoulos S, Rizzoli R (2013) Association of circulating sclerostin with bone mineral mass, microstructure, and turnover biochemical markers in healthy elderly men and women. J Clin Endocrinol Metab 98:3873–3883
Acknowledgments
This study was supported by the National Institutes of Health grants RC1 AR058405 to TML and R01 AR060700 to AJB and the Erwin Schroedinger grant (J-3079 to JMP). We thank Thelma Munoz and Melissa Guan for their help in recruiting and consenting the patients. We also would like to thank Elzbieta Dworakowski and Serge Cremers (Columbia University) for the analysis of serum sclerostin levels which was supported by the National Center for Advancing Translational Sciences, National Institutes of Health through grant number UL1 TR000040 (PI Henry Ginsberg).
Conflict of interest
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Heilmeier, U., Carpenter, D.R., Patsch, J.M. et al. Volumetric femoral BMD, bone geometry, and serum sclerostin levels differ between type 2 diabetic postmenopausal women with and without fragility fractures. Osteoporos Int 26, 1283–1293 (2015). https://doi.org/10.1007/s00198-014-2988-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-014-2988-7