
Abstract
Summary
In this cross-sectional study, we found that areal bone mineral density (aBMD) at the knee and specific tibia bone geometry variables are associated with fragility fractures in men and women with chronic spinal cord injury (SCI).
Introduction
Low aBMD of the hip and knee regions have been associated with fractures among individuals with chronic motor complete SCI; however, it is unclear whether these variables can be used to identify those at risk of fracture. In this cross-sectional study, we examined whether BMD and geometry measures are associated with lower extremity fragility fractures in individuals with chronic SCI.
Methods
Adults with chronic [duration of injury ≥ 2 years] traumatic SCI (C1-L1 American Spinal Cord Injury Association Impairment Scale A-D) reported post injury lower extremity fragility fractures. Dual-energy X-ray absorptiometry (DXA) was used to measure aBMD of the hip, distal femur, and proximal tibia regions, while bone geometry at the tibia was assessed using peripheral quantitative computed tomography (pQCT). Logistic regression and univariate analyses were used to identify whether clinical characteristics or bone geometry variables were associated with fractures.
Results
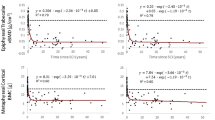
Seventy individuals with SCI [mean age (standard deviation [SD]), 48.8 (11.5); 20 females] reported 19 fragility fractures. Individuals without fractures had significantly greater aBMD of the hip and knee regions and indices of bone geometry. Every SD decrease in aBMD of the distal femur and proximal tibia, trabecular volumetric bone mineral density, and polar moment of inertia was associated with fracture prevalence after adjusting for motor complete injury (odds ratio ranged from 3.2 to 6.1).
Conclusion
Low knee aBMD and suboptimal bone geometry are significantly associated with fractures. Prospective studies are necessary to confirm the bone parameters reported to predict fracture risk in individuals with low bone mass and chronic SCI.


Similar content being viewed by others

References
Garland DE, Adkins RH (2001) Bone loss at the knee in spinal cord injury. Top Spinal Cord Inj Rehabil 6:37–46
Garland DE, Stewart CA, Adkins RH et al (1992) Osteoporosis after spinal cord injury. J Orthop Res 10:371–378
Zehnder Y, Lüthi M, Michel D et al (2004) Long-term changes in bone metabolism, bone mineral density, quantitative ultrasound parameters, and fracture incidence after spinal cord injury: a cross-sectional observational study in 100 paraplegic men. Osteoporos Int 15:180–189
Vestergaard P, Krogh K, Rejnmark L et al (1998) Fracture rates and risk factors for fractures in patients with spinal cord injury. Spinal Cord 36:790–796
Ragnarsson KT, Sell GH (1981) Lower extremity fractures after spinal cord injury: a retrospective study. Arch Phys Med Rehabil 62:418–423
Comarr AE, Hutchinson RH, Bors E (2005) Extremity fractures of patients with spinal cord injuries. Top Spinal Cord Inj Rehabil 11:1–10
Freehafer AA, Hazel CM, Becker CL (1981) Lower extremity fractures in patients with spinal cord injury. Spinal Cord 19:367–372
Lazo MG, Shirazi P, Sam M et al (2001) Osteoporosis and risk of fracture in men with spinal cord injury. Spinal Cord 39:208–214
Carbone LD, Chin AS, Burns SP et al (2013) Morbidity following lower extremity fractures in men with spinal cord injury. Osteoporos Int. doi:10.1007/s00198-013-2295-8
World Health Organization (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 843:1–129
Papaioannou A, Morin S, Cheung AM et al (2010) 2010 clinical practice guidelines for the diagnosis and management of osteoporosis in Canada: summary. Can Med Assoc J 182:1864–1873
Kanis JA, Johnell O, Odén A et al (2008) FRAX™ and the assessment of fracture probability in men and women from the UK. Osteoporos Int 19:385–397
Farry A, Baxter D (2010) The incidence and prevalence of spinal cord injury in Canada. Overview and estimates based on current evidence. Rick Hansen Institute and Urban Futures
Craven B, Giangregorio L, Robertson L et al (2008) Sublesional osteoporosis prevention, detection, and treatment: a decision guide for rehabilitation clinicians treating patients with spinal cord injury. Crit Rev Phys Rehabil Med 20:277–321
Eser P, Frotzler A, Zehnder Y et al (2004) Relationship between the duration of paralysis and bone structure: a pQCT study of spinal cord injured individuals. Bone 34:869–880
Slade JM, Bickel CS, Modlesky CM et al (2005) Trabecular bone is more deteriorated in spinal cord injured versus estrogen-free postmenopausal women. Osteoporos Int 16:263–272
Modlesky CM, Majumdar S, Narasimhan A, Dudley GA (2004) Trabecular bone microarchitecture is deteriorated in men with spinal cord injury. J Bone Miner Res 19:48–55
Biering-Sorensen F, Bohr HH, Schaadt OP (1990) Longitudinal study of bone mineral content in the lumbar spine, the forearm and the lower extremities after spinal cord injury. Eur J Clin Investig 20:330–335
Garland DE, Adkins RH, Stewart CA (2005) Fracture threshold and risk for osteoporosis and pathologic fractures in individuals with spinal cord injury. Top Spinal Cord Inj Rehabil 11:61–69
Eser P, Frotzler A, Zehnder Y, Denoth J (2005) Fracture threshold in the femur and tibia of people with spinal cord injury as determined by peripheral quantitative computed tomography. Arch Phys Med Rehabil 86:498–504
Sheu Y, Zmuda JM, Boudreau RM et al (2011) Bone strength measured by peripheral quantitative computed tomography and the risk of nonvertebral fractures: the osteoporotic fractures in men (MrOS) study. J Bone Miner Res 26:63–71
Jamal SA, Gilbert J, Gordon C, Bauer DC (2006) Cortical pQCT measures are associated with fractures in dialysis patients. J Bone Miner Res 21:543–548
Taes Y, Lapauw B, Griet V et al (2010) Prevalent fractures are related to cortical bone geometry in young healthy men at age of peak bone mass. J Bone Miner Res 25:1433–1440
Frey-Rindova P, De Bruin ED, Stüssi E et al (2000) Bone mineral density in upper and lower extremities during 12 months after spinal cord injury measured by peripheral quantitative computed tomography. Spinal Cord 38:26–32
Dionyssiotis Y, Trovas G, Galanos A et al (2007) Bone loss and mechanical properties of tibia in spinal cord injured men. J Musculoskelet Neuronal Interact 7:62–68
Maynard FM Jr, Bracken MB, Creasey G et al (1997) International standards for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Spinal Cord 35:266–274
Edwards LA, Bugaresti JM, Buchholz AC (2008) Visceral adipose tissue and the ratio of visceral to subcutaneous adipose tissue are greater in adults with than in those without spinal cord injury, despite matching waist circumferences. Am J Clin Nutr 87:600–607
Krieger N, Tenenhouse A, Joseph L et al (1999) The Canadian Multicentre Osteoporosis Study. Can J Aging 18:376–387
Moreno JC (2001) Protocol for using dual photon absorptiometry software to measure BMD of distal femur and proximal tibia. Master’s thesis, McMaster University, Hamilton
Yoshioka Y, Siu DW, Scudamore RA, Cooke TD (1989) Tibial anatomy and functional axes. J Orthop Res 7:132–137
Giangregorio L, Lala D, Hummel K et al (2012) Measuring apparent trabecular density and bone structure using peripheral quantitative computed tomography at the tibia: precision in participants with and without spinal cord injury. J Clin Densitom. doi:10.1016/j.jocd.2012.02.003
Ashe MC, Khan KM, Kontulainen SA et al (2006) Accuracy of pQCT for evaluating the aged human radius: an ashing, histomorphometry and failure load investigation. Osteoporos Int 17:1241–1251
Melton LJ, Beck TJ, Amin S et al (2005) Contributions of bone density and structure to fracture risk assessment in men and women. Osteoporos Int 16:460–467
Garland DE, Adkins RH, Kushwaha V et al (2004) Risk factors for osteoporosis at the knee in the spinal cord injury population. J Spinal Cord Med 27:202–206
Frost HM (2003) Bone’s mechanostat: a 2003 update. Anat Rec A Discov Mol Cell Evol Biol 275:1081–1101
Totosy de Zepetnek JO, Craven BC, Giangregorio LM (2012) An evaluation of the muscle–bone unit theory among individuals with chronic spinal cord injury. Spinal Cord 50:147–152
De Bruin ED, Herzog R, Rozendal RH et al (2000) Estimation of geometric properties of cortical bone in spinal cord injury. Arch Phys Med Rehabil 81:150–156
Jiang S-D, Dai L-Y, Jiang L-S (2006) Osteoporosis after spinal cord injury. Osteoporos Int 17:180–192. doi:10.1007/s00198-005-2028-8
Duan Y, De Luca V, Seeman E (1999) Parathyroid hormone deficiency and excess: similar effects on trabecular bone but differing effects on cortical bone. J Clin Endocrinol Metab 84:718–722
Lips P (2001) Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev 22:477–501
Negri AL, Barone R, Lombas C et al (2006) Evaluation of cortical bone by peripheral quantitative computed tomography in continuous ambulatory peritoneal dialysis patients. Hemodial Int 10:351–355
Bauman WA, Zhong YG, Schwartz E (1995) Vitamin D deficiency in veterans with chronic spinal cord injury. Metabolism 44:1612–1616
Hummel K, Craven BC, Giangregorio L (2012) Serum 25(OH)D, PTH and correlates of suboptimal 25(OH)D levels in persons with chronic spinal cord injury. Spinal Cord 50:812–816
Bauman WA, Spungen AM (2000) Metabolic changes in persons after spinal cord injury. Phys Med Rehabil Clin N Am 11:109–140
Acknowledgments
The authors acknowledge the support from the Ontario Neurotrauma Foundation (grant #2009-SC-MA-684), the Canadian Institutes of Health Research (grant #86521), the Spinal Cord Injury Solutions Network (RHI; grant #2010-43), and the Toronto Rehabilitation Institute who receives funding under the Provincial Rehabilitation Research Program from the Ministry of Health and Long-Term Care. The views expressed do not necessarily reflect those of the ministry.
Conflicts of interest
A. Papiaoannou, JD. Adachi - Consultant/Speaker: Amgen, Eli Lillly, GSK, Merk, Novartis, Warner-Chilcott; Clinic Trials: Eli Lilly, Merck, Novartism, Pfizer.
M. Popovic - Share holder in MyndTec.
L. Giangregorio - Research Support: Merck.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lala, D., Craven, B.C., Thabane, L. et al. Exploring the determinants of fracture risk among individuals with spinal cord injury. Osteoporos Int 25, 177–185 (2014). https://doi.org/10.1007/s00198-013-2419-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-013-2419-1