
Abstract
Summary
This study assesses the costs of non-vertebral osteoporosis-related fractures patients compared with osteoporosis patients without fractures, focusing on the second year following a fracture. Since fracture patients remained more costly in the second year, their economic burden extends beyond the year in which the fracture occurs.
Introduction
The purpose of this study is to examine the comorbidity profile, resource use, and direct costs of patients who incur osteoporosis-related non-vertebral (NV) fractures in the United States during the 2 years following an incident fracture, focusing on the second year following a fracture.
Methods
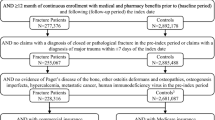
Osteoporosis patients (ICD-9-CM: 733.0) with a NV fracture (hip, femur, pelvis, lower leg, upper arm, forearm, rib, and multiple sites) were selected from a privately insured health insurance claims database (>8 million lives, ages 18–64, 1999–2006). These NV fracture patients were randomly matched 1:1 on age, gender, employment status, and geographic region to controls with osteoporosis but without a fracture history. Year-by-year and month-by-month rates of comorbidities, resource use, and direct costs were calculated for the matched sample (N = 3,781).
Results
Comorbidity rates and resource use remained significantly higher among NV fracture patients during second year following an NV fracture compared with controls, although absolute rates of comorbidities and service utilization declined. Mean direct excess costs for NV fracture patients fell from $5,267 in the first year to $2,072 in the second year after a fracture, but remained statistically significant (p < 0.01). Patients with fractures of the pelvis, hip, and femur had the highest excess costs in the second year ($5,121, $3,930, and $3,828, respectively). Although hip fractures had highest excess costs over both years, non-vertebral, non-hip fracture patients made up a larger proportion of the sample and were significantly more costly than controls.
Conclusions
Patients with osteoporosis-related NV fractures have substantial excess costs beyond the first year in which the fracture occurs.



Similar content being viewed by others


References
Boonen S, Singer AJ (2008) Osteoporosis management: impact of fracture type on cost and quality of life in patients at risk for fracture I. Curr Med Res Opin 24(6):1781–1788
Orsini LS, Rousculp MD, Long SR, Wang S (2005) Health care utilization and expenditures in the United States: a study of osteoporosis-related fractures. Osteoporos Int 16(4):359–371
National Osteoporosis Foundation. Osteoporosis Fast Facts. http://www.nof.org/osteoporosis/diseasefacts.htm. Accessed 20 Aug 2009
World Health Organization (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. WHO Technical Report Series, No. 843. Geneva
International Osteoporosis Foundation. Facts and statistics about osteoporosis and its impact. http://www.iofbonehealth.org/facts-and-statistics.html. Accessed 08 Oct 2009
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22:465–475
Ohlsfeldt RL, Borisov NN, Steer RL (2006) Fragility fracture-related direct medical costs in the first year following a nonvertebral fracture in a managed care setting. Osteoporos Int 17:252–258
Ray NF, Chan JK, Thamer M, Melton LJ 3rd (1997) Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res 12(1):24–35
Pike C, Birnbaum H, Schiller M, Sharma H, Burge RT, Edgell ET (2010) Direct and indirect costs of non-vertebral fracture patients with osteoporosis in the U.S. Pharmacoeconomics 28:395–409
Levy P, Levy E, Audran M, Cohen-Solal M, Fardellone P, Le Parc JM (2002) The cost of osteoporosis in men: the French situation. Bone 30(4):631–636
Bouee S, Lafuma A, Fagnani F, Meunier PJ, Reginster JY (2006) Estimation of direct unit costs associated with non-vertebral osteoporotic fractures in five European countries. Rheumatol Int 26(12):1063–1072
Chen Z, Maricic M, Aragaki AK, Mouton C, Arendell L, Lopez AM, Bassford T, Chlebowsk RT (2009) Fracture risk increases after diagnosis of breast or other cancers in postmenopausal women: results from the Women’s Health Initiative. Osteoporos Int 20(4):527–536
Melton LJ, Gabriel SE, Crowson CS, Tosteson AN, Johnell O, Kanis JA (2003) Cost-equivalence of different osteoporotic fractures. Osteoporos Int 14(5):383–388
Melton LJ (2003) Adverse outcomes of osteoporotic fractures in the general population. J Bone Miner Res 18(6):1139–1141
Lindsay R, Burge RT, Strauss M (2005) One year outcomes and costs following a vertebral fracture. Osteoporos Int 16:78–85
Tosteson AN, Gabriel SE, Grove MR, Moncur MM, Kneeland TS, Melton LJ 3rd (2001) Impact of hip and vertebral fractures on quality-adjusted life years. Osteoporos Int 12(12):1042–1049
Owen RA, Melton LJ, Gallagher JC, Riggs BL (1980) The national cost of acute care of hip fractures associated with osteoporosis. Clin Orthop Relat Res 150:172–176
Chen Z, Maricic M, Aragaki AK, Mouton C, Arendell L, Lopez AM, Bassford T, Chlebowski RT (2009) Fracture risk increases after diagnosis of breast or other cancers in postmenopausal women: results from the Women’s Health Initiative. Osteoporos Int 20(4):527–536
Abelson A (2008) A review of Paget’s disease of bone with a focus on the efficacy and safety of zoledronic acid 5 mg. Curr Med Res Opin 24(3):695–705
Blouin S, Libouban H, Moreau MF, Chappard D (2008) Orchidectomy models of osteoporosis. Methods Mol Bio 455:125–134
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis 40(5):373–383
Romano PS, Roos LL, Jollis J (1993) Adapting a clinical comorbidity index for use with ICD-9-CM administrative data. J Clin Epidemiol 46(10):1075–1079
Lyles KW, Schenck AP, Colon-Emeric CS (2008) Hip and other osteoporotic fractures increase the risk of subsequent fractures in nursing home residents. Osteoporos Int 19(8):1225–1233
Kanis JA (2009) FRAX WHO Fracture Risk Assessment Tool. World Health Organization Collaborating Center for Metabolic Bone Diseases, University of Sheffield. http://www.shef.ac.uk/FRAX/. Accessed 10 Sep 2009
Nguyen TV, Center JR, Eisman JA (2004) Osteoporosis: underrated, underdiagnosed and undertreated. Med J Aust 180(5 Suppl):S18–S22
Vestergaard P, Renjnmark L, Mosekilde L (2005) Osteoporosis is markedly underdiagnosed: a nationwide study from Denmark. Osteoporos Int 16(2):134–141
Westesson PL, Lee RK, Ketkar MA, Lin EP (2002) Underdiagnosis and undertreatment of osteoporosis. Lancet 360(9348):1891
Gunter MJ, Beaton SJ, Brenneman SK, Chen YT, Abbott TA 3rd, Gleeson JM (2003) Management of osteoporosis in women aged 50 and older with osteoporosis-related fractures in a managed care population. Dis Manag 6(2):83–91
Sasser AC, Rousculp MD, Birnbaum HG, Oster EF, Lufkin E, Mallet D (2005) Economic burden of osteoporosis, breast cancer, and cardiovascular disease among postmenopausal women in an employed population. Womens Health Issues 15(3):97–108
Kowalski SC, Sjenzfeld VL, Ferraz MB (2004) Resource utilization in postmenopausal osteoporosis without incident fractures. J Rheumatol 31:938–942
Rabenda V, Manette C, Lemmens R, Mariani A-M, Struvay N, Reginster J-Y (2006) The direct and indirect costs of the chronic management of osteoporosis: a prospective follow-up of 3440 active subjects. Osteoporos Int 17:1346–1352
Seeman E (2007) Unmet needs in fracture prevention: new European guidelines for the investigation and registration of therapeutic agents. Osteoporos Int 18(5):569–573
Acknowledgments
We thank Dr Susan Dennett of Eli Lilly and Company for her contributions to the study design. We also thank Dr Anna Gu and Hari Sharma for providing computer programming input on various aspects of the analysis.
Conflict of interest
This research project was funded by Eli Lilly and Company. Drs. Russel Burge and Eric Edgell are employees of Eli Lilly and Company in the Global Health Outcomes department. Eli Lilly and Company markets pharmacological therapies for the prevention and treatment of osteoporosis.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary materials
ESM 1
(PDF 23 kb)
Rights and permissions
About this article
Cite this article
Pike, C., Birnbaum, H.G., Schiller, M. et al. Economic burden of privately insured non-vertebral fracture patients with osteoporosis over a 2-year period in the US. Osteoporos Int 22, 47–56 (2011). https://doi.org/10.1007/s00198-010-1267-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-010-1267-5