
Abstract
Summary
The effects of teriparatide versus alendronate were compared by gender and menopausal status in patients with glucocorticoid-induced osteoporosis. At 18 months, increases in lumbar spine BMD were significantly greater in the teriparatide versus alendronate group in postmenopausal women (7.8% versus 3.7%, p < 0.001), premenopausal women (7.0% versus 0.7%, p < 0.001), and men (7.3% versus 3.7%, p = 0.03).
Introduction
In patients with glucocorticoid-induced osteoporosis (GIO), teriparatide significantly increased bone mineral density (BMD) and decreased vertebral fractures compared with alendronate. We examined effects of teriparatide versus alendronate by gender and menopausal status.
Methods
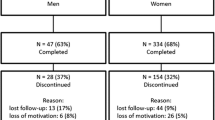
This was a multicenter, randomized, double-blind study of teriparatide 20 µg/day versus alendronate 10 mg/day in patients with GIO (277 postmenopausal women, 67 premenopausal women, 83 men). Primary outcome was change in lumbar spine BMD. Secondary outcomes included change in hip BMD, change in bone biomarkers, fracture incidence, and safety.
Results
At 18 months, mean percent increases from baseline in lumbar spine BMD were significantly greater in the teriparatide versus alendronate group in postmenopausal women (7.8% versus 3.7%, p < 0.001), premenopausal women (7.0% versus 0.7%, p < 0.001), and men (7.3% versus 3.7%, p = 0.03). Radiographic vertebral fractures occurred in one teriparatide (one postmenopausal) and ten alendronate patients (six postmenopausal, four men), and nonvertebral fractures occurred in 12 teriparatide (nine postmenopausal, two premenopausal, one man) and eight alendronate patients (six postmenopausal, two men). The proportion of patients reporting adverse events in teriparatide versus alendronate groups was consistent across subgroups.
Conclusion
Among men and pre- and postmenopausal women with GIO, lumbar spine BMD increased more in patients receiving teriparatide compared with alendronate.



Similar content being viewed by others


References
Van Staa TP, Leufkens HGM, Abenhaim L et al (2000) Use of oral corticosteroids and risk for fractures. J Bone Miner Res 15:993–1000
Saag KG (2003) Glucocorticoid-induced osteoporosis. Endocrinol Metab Clin North Am 32:135–157
Canalis E, Mazziotti G, Giustina A et al (2004) Glucocorticoid-induced osteoporosis: pathophysiology and perspective. Osteoporos Int 18:1319–1328
Kanis JA, Johansson H, Oden A et al (2004) A meta-analysis of prior corticosteroid use and fracture risk. J Bone Miner Res 19:893–899
Weinstein RS, Jilka RL, Parfitt AM et al (1998) Inhibition of osteoblastogenesis and promotion of apoptosis of osteoblasts and osteocytes by glucocorticoids. Potential mechanisms of their deleterious effects on bone. J Clin Invest 102:274–282
Rubin MR, Bilezikian JP (2002) The role of parathyroid hormone in the pathogenesis of glucocorticoid-induced osteoporosis: a reexamination of the evidence. J Clin Endocrinol Metab 87:4033–4041
Schakman O, Gilson H, Thissen JP (2008) Mechanism of glucocorticoid-induced myopathy. J Endocrinol 197:1–10
American College of Rheumatology (2001) Recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis: 2001 update. American College of Rheumatology Ad Hoc Committee on Glucocorticoid-Induced Osteoporosis. Arthritis Rheum 44:1496–1503
Sambrook PN, Diamond T, Ferris L et al (2001) Corticosteroid induced osteoporosis. Guidelines for treatment. Aust Fam Physician 30:793–796
Royal College of Physicians (2002) Glucocorticoid-induced osteoporosis: guidelines for prevention and treatment. London, UK. http://www.rcplondon.ac.uk/pubs/books/glucocorticoid/index.asp
Adler RA, Hochberg MC (2003) Suggested guidelines for evaluation and treatment of glucocorticoid-induced osteoporosis for the Department of Veterans Affairs. Arch Intern Med 163:2619–2624
Geusens PP, de Nijs RN, Lems WF et al (2004) Prevention of glucocorticoid osteoporosis: a consensus document of the Dutch Society for Rheumatology. Ann Rheum Dis 63:324–325
Nawata H, Soen S, Takayanagi R et al (2005) Guidelines on the management and treatment of glucocorticoid-induced osteoporosis of the Japanese Society for Bone and Mineral Research. J Bone Miner Metab 23:105–109
Devogelaer JP, Goemaere S, Boonen S et al (2006) Evidence-based guidelines for the prevention and treatment of glucocorticoid-induced osteoporosis: a consensus document of the Belgian Bone Club. Osteoporos Int 17:8–19
Rogers MJ, Frith JC, Luckman SP et al (1999) Molecular mechanisms of action of bisphosphonates. Bone 24:73S–79S
Dobnig H, Turner RT (1995) Evidence that intermittent treatment with parathyroid hormone increases bone formation in adult rats by activation of bone lining cells. Endocrinology 136:3632–3638
Jilka RL, Weinstein RS, Bellido T et al (1999) Increased bone formation by prevention of osteoblast apoptosis with parathyroid hormone. J Clin Invest 104:439–446
Canalis E, Giustina A, Bilezikian JP (2007) Mechanisms of anabolic therapies for osteoporosis. N Engl J Med 357:905–916
Goltzman D (2008) Studies on the mechanisms of the skeletal anabolic action of endogenous and exogenous parathyroid hormone. Arch Biochem Biophys 473:218–224
Saag KG, Shane ES, Boonen S et al (2007) Teriparatide or alendronate in glucocorticoid-induced osteoporosis. New Eng J Med 357:2028–2039
Genant HK, Jergas M, Palermo L et al (1996) Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis. J Bone Miner Res 11:984–996
Saag KG, Emkey R, Schnitzer TJ et al (1998) Alendronate for the prevention and treatment of glucocorticoid-induced osteoporosis. N Engl J Med 339:292–299
Adachi JD, Saag KG, Delmas PD et al (2001) Two year effects of alendronate on bone mineral density and vertebral fracture in patients receiving glucocorticoids: a randomized, double blind, placebo controlled extension trial. Arthritis Rheum 44:202–211
Cohen S, Levy RM, Keller M et al (1999) Risedronate therapy prevents corticosteroid-induced bone loss: a twelve-month, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum 42:2309–2318
Reid DM, Hughes RA, Laan RF et al (2000) Efficacy and safety of daily risedronate in the treatment of corticosteroid-induced osteoporosis in men and women: a randomized trial. J Bone Miner Res 15:1006–1013
Ringe JD, Dorst A, Faber H et al (2003) Intermittent intravenous ibandronate injections reduce vertebral fracture risk in corticosteroid-induced osteoporosis: results from a long-term comparative study. Osteoporos Int 14(10):801–807
Wallach S, Cohen S, Reid DM et al (2000) Effects of risedronate treatment on bone density and vertebral fracture in patients on corticoid therapy. Calcif Tissue Int 67:277–285
Lems WF, Lodder MC, Lips P et al (2006) Positive effects of alendronate on bone mineral density and markers of bone turnover in patients with rheumatoid arthritis on chronic treatment with low-dose prednisone: a randomized, double-blind, placebo-controlled trial. Osteoporos Int 17:716–723
de Nijs RN, Jacobs JW, Lems WF et al (2006) Alendronate or alfacalcidol in glucocorticoid-induced osteoporosis. N Engl J Med 355:675–684
Sambrook PN (2007) Anabolic therapy in glucocorticoid-induced osteoporosis. N Engl J Med 357:2084–2086
Lane NE, Sanchez S, Modin GW et al (1998) Parathyroid hormone treatment can reverse corticosteroid-induced osteoporosis. Results of a randomized controlled clinical trial. J Clin Invest 102:1627–1633
Rehman Q, Lang TF, Arnaud CD et al (2003) Daily treatment with parathyroid hormone is associated with an increase in vertebral cross-sectional area in postmenopausal women with glucocorticoid-induced osteoporosis. Osteoporos Int 14:77–81
Chen P, Miller PD, Recker R et al (2007) Increases in BMD correlate with improvements in bone microarchitecture with teriparatide treatment in postmenopausal women with osteoporosis. J Bone Miner Res 22:1173–1180
Cummings SR, Karpf DB, Harris F et al (2002) Improvement in spine bone density and reduction in risk of vertebral fractures during treatment with antiresorptive drugs. Am J Med 112:281–289
Li Z, Meredith MP, Hoseyni MS (2001) A method to assess the proportion of treatment effect explained by a surrogate endpoint. Statist Med 20:3175–3188
Keaveny TM, Donley DW, Hoffmann PF, Mitlak BH, Glass EV, San Martin JA (2007) Effects of teriparatide and alendronate on vertebral strength as assessed by finite element modeling of QCT scans in women with osteoporosis. J Bone Miner Res 21:149–157
Ramsey-Goldman R, Dunn JE, Huang CF et al (1999) Frequency of fractures in women with systemic lupus erythematosus: comparison with United States population data. Arthritis Rheum 42:882–890
Steinbuch M, Youket TE, Cohen S (2004) Oral glucocorticoid use is associated with an increased risk of fracture. Osteoporos Int 15:323–328
Klaus J, Armbrecht G, Steinkamp M et al (2002) High prevalence of osteoporotic vertebral fractures in patients with Crohn's disease. Gut 51:654–658
Neer RM, Arnaud CD, Zanchetta JR et al (2001) Effect of parathyroid hormone(1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 344(19):1434–1441
Orwoll ES, Scheele WH, Paul S et al (2003) The effect of teriparatide [human parathyroid hormone (1–34)] therapy on bone density in men with osteoporosis. J Bone Miner Res 18:9–17
Liberman UA, Weiss SR, Bröll J et al (1995) Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. N Engl J Med 333:1437–1443
McDonough AK, Curtis JR, Saag KG (2008) The epidemiology of glucocorticoid-associated adverse events. Curr Opin Rheumatol 20:131–137
Acknowledgments
This study was supported by Eli Lilly and Company. The authors acknowledge the study investigators [20] and also acknowledge JoNita Cogburn, Ph.D., i3 Statprobe for editorial assistance.
Conflicts of interest
BL Langdahl is a lecturer for Eli Lilly and Company, Novartis, Amgen, Servier, Roche, and Merck Sharp & Dohme and serves on advisory boards for Eli Lilly and Company, Novartis, and Amgen.
E Shane receives research support from Novartis and Eli Lilly and Company.
H Dobnig is a lecturer at symposia organized by Eli Lilly and Company.
JR Zanchetta has received consultant fees and/or research grants from Sanofi-Aventis, GlaxoSmithKline, MSD, Eli Lilly and Company, Wyeth, Amgen, Pfizer, Roche, and Servier.
M Maricic is a lecturer for and has received research grant support from Eli Lilly and Company.
F Marin, K Krohn, K See, and MR Warner are employees and stockholders of Eli Lilly and Company.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Langdahl, B.L., Marin, F., Shane, E. et al. Teriparatide versus alendronate for treating glucocorticoid-induced osteoporosis: an analysis by gender and menopausal status. Osteoporos Int 20, 2095–2104 (2009). https://doi.org/10.1007/s00198-009-0917-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-009-0917-y