
Abstract
Introduction
The terminology for female pelvic floor prolapse (POP) should be defined and organized in a clinically-based consensus Report.
Methods
This Report combines the input of members of two International Organizations, the International Urogynecological Association (IUGA) and the International Continence Society (ICS), assisted at intervals by external referees. Appropriate core clinical categories and a sub-classification were developed to give a coding to definitions. An extensive process of fourteen rounds of internal and external review was involved to exhaustively examine each definition, with decision-making by collective opinion (consensus).
Results
A Terminology Report for female POP, encompassing over 230 separate definitions, has been developed. It is clinically-based with the most common diagnoses defined. Clarity and user-friendliness have been key aims to make it interpretable by practitioners and trainees in all the different specialty groups involved in female pelvic floor dysfunction and POP. Female-specific imaging (ultrasound, radiology and MRI) and conservative and surgical managements are major additions and appropriate figures have been included to supplement and clarify the text. Emerging concepts and measurements, in use in the literature and offering further research potential, but requiring further validation, have been included as an appendix. Interval (5–10 year) review is anticipated to keep the document updated and as widely acceptable as possible.
Conclusion
A consensus-based Terminology Report for female POP has been produced to aid clinical practice and research.
Introduction
Prolapse (Latin: Prolapsus – “a slipping forth”) refers to a falling, slipping or downward displacement of a part or organ. Pelvic organ refers most commonly to the uterus and/or the different vaginal compartments and their neighboring organs such as bladder, rectum or bowel. Pelvic organ prolapse (POP) is thus, primarily, a definition of anatomical change. Some such changes may well be considered within the range of normality for certain women. A diagnosis of POP ideally demands clear clinical evidence, starting with a woman having symptoms related to the “downward displacement” of a pelvic organ.
There is currently no single document encompassing all elements required for diagnoses in the area of female POP. Such a report would require a full outline of the terminology for symptoms, signs, clinical assessments, functional investigations for female POP, the imaging associated with those investigations, the most common diagnoses and terminology for the different conservative and surgical treatment modalities.
There will be a need to reference considerably the 2010 IUGA-ICS Joint Terminology Report on Female Pelvic Floor Dysfunction [1]. An original aim of that report [1] had been to provide a general terminology, forming a “backbone” or “core” terminology to which more specific terminologies can be attached. Reference can also be made to three other published Standardization Reports [2–4] and 6 joint IUGA-ICS Female Terminology Reports [5–10] subsequent to the 2010 Report [1], three published [5–7], three [8–10] advanced in development.
In terms of the previous standardization document on female POP [4], now 20 years old, there has been much discussion and debate [11–14] on the possible need to update its classification POP-Q, or at least to present it in a refreshed version. The POP Working Group has opted for the latter, with major upgrades to symptoms, signs, investigations and diagnoses, but a conservative approach to the classification itself (apart from adding a validated simplified version), due to the longevity of its use and the lack of any validated, clearly superior alternative classification. Female-specific imaging (ultrasound, radiology and MRI) and conservative and surgical managements are major additions and appropriate figures have been included to supplement and clarify the text. Emerging concepts and measurements, in use in the literature and offering further research potential, but requiring further validation, have been included as an Appendix. This Report acknowledges that POP is often not a diagnosis in isolation but may be associated with POP-related and unrelated voiding, defecatory and/or sexual dysfunctions and/or other diagnoses of pelvic floor dysfunction.
This Terminology Report is inherently and appropriately a definitional document, collating the definitions of those terms, i.e., “words used to express a defined concept in a particular branch of study” [15], here POP. Emphasis has been on comprehensively including those terms in current use in the relevant peer-reviewed literature. The aim is to assist clinical practice and research. Some new and revised terms have been included. Explanatory notes on definitions have been referred, where possible, to the “Footnotes” section.
Like all the other joint IUGA-ICS female-specific terminology reports, every effort has been made to ensure this Report is:
-
(1)
User-friendly: It should be able to be understood by all clinical and research users.
-
(2)
Clinically-based: Symptoms, signs and validated assessments/investigations should be presented for use in forming workable diagnoses for POP and associated dysfunctions. “Symptoms”, “Signs”, “Prolapse quantification”, “Investigations” and “Prolapse imaging” sections will address symptoms, signs, POP quantification, investigations for associated dysfunctions and current POP imaging modalities that may be used to make those diagnoses. A number of related radiological investigations including Magnetic Resonance Imaging (MRI) and Computerized Tomography (CT) have also been incorporated. “Diagnoses” section will address POP diagnoses, possible POP-related diagnoses and co-existing diagnoses. The scope of the Report will exclude more invasive investigations requiring an anesthetic. “Conservative treatments” and “Surgical treatments” sections will list the terminology for evidence-based conservative and surgical treatments for POP.
-
(3)
Origin: Where a term’s existing definition (from one of multiple sources used) is deemed appropriate, that definition will be included and duly referenced. A large number of terms in female pelvic floor prolapse and dysfunction, because of their long-term use, have now become generic, as apparent by their listing in medical dictionaries.
-
(4)
Able to provide explanations: Where a specific explanation is deemed appropriate to describe a change from earlier definitions or to qualify the current definition, this will be included as an addendum to this paper.Footnote 1 , Footnote 2 , Footnote 3 Wherever possible, evidence-based medical principles will be followed.
It is suggested that acknowledgement of these standards in written publications related to female POP, be indicated by a footnote to the section “Methods and Materials” or its equivalent, to read as follows: “Methods, definitions and units conform to the standards jointly recommended by the International Urogynecological Association and the International Continence Society except where specifically noted”.
Symptoms
Symptom: Any morbid phenomenon or departure from the normal in structure, function or sensation, experienced by the woman and indicative of disease or a health problem [16]. Symptoms are either volunteered by, or elicited from the woman or may be described by the woman’s caregiver [1–3].
Pelvic organ prolapse (POP) symptoms
Prolapse symptoms [1]: A departure from normal sensation, structure or function, experienced by the woman in reference to the position of her pelvic organs. Symptoms are generally worse in situations when gravity might make the prolapse worse (e.g., after long periods of standing or exercise) and better when gravity is not a factor e.g., lying supine. Again symptoms may be more noticeable at times of abdominal straining e.g., defecation.
A: Vaginal prolapse symptoms
-
(i)
Vaginal bulging [1]: Complaint of a “bulge”, lump or “something coming down” or “falling out” through the vaginal introitus.
The woman may state she can either feel the bulge by direct palpation or see it, perhaps aided with a mirror1.
-
(ii)
Pelvic pressure [1]: Complaint of increased heaviness or dragging (pain or discomfort) in the suprapubic area and/or pelvis.
-
(iii)
Bleeding, discharge, infection [1]: Complaint of abnormal vaginal bleeding, discharge or infection which may be related to ulceration of the prolapse.
-
(iv)
Splinting / Digitation [1]: Complaint of the need to digitally replace the prolapse or to otherwise apply manual pressure, e.g., to the vagina, perineum or perianal area (splinting), or rectally (digitation) to assist voiding or defecation.
-
(v)
Low backache [1] (POP-related): Complaint of low, sacral (or “menstrual-like”) backache associated temporally with vaginal POP and relieved when prolapse is reduced.
B: Urinary tract prolapse symptoms
-
(i)
Urethral Prolapse: Complaint of a “lump” at the external urethral meatus.
C: Anorectal prolapse symptoms
-
(i)
Anorectal prolapse: Complaint of a “bulge” or “something coming down” towards or through the anus/rectum. The woman may state she can either feel the bulge by direct palpation or see it perhaps aided with a mirror1.
-
(ii)
Rectal prolapse: Complaint of external protrusion of the rectum.
Effects of pelvic organ prolapse on bladder, bowel and sexual function
As demonstrated in Fig. 1, higher stage utero-vaginal prolapse will usually cause anatomical distortion to surrounding organs, bladder and rectum most commonly. This can lead to abnormal function, most commonly difficulty with bladder and bowel emptying. Commonly, symptoms related to those surrounding organs are the most bothersome leading to the eventual diagnosis of the POP.

Utero-vaginal prolapse
D: Potential prolapse-related lower urinary tract symptoms
-
(i)
Hesitancy [1]: Complaint of a delay in initiating micturition.
-
(ii)
Slow stream [1]: Complaint of a urinary stream perceived as slower compared to previous performance (particularly prior to the development of POP) or in comparison with others.
-
(iii)
Intermittency [1]: Complaint of urine flow that stops and starts on one or more occasions during voiding.
-
(iv)
Straining to void [1]: Complaint of the need to make an intensive effort (by abdominal straining, Valsalva or suprapubic pressure) to either initiate, maintain or improve the urinary stream.
-
(v)
Spraying (splitting) of urinary stream [1]: Complaint that the urine stream is a spray or split rather than a single discrete stream.
-
(vi)
Feeling of incomplete (bladder) emptying [1]: Complaint that the bladder does not feel empty after micturition.
-
(vii)
Need to immediately re-void [1]: Complaint that further micturition is necessary soon after passing urine.
-
(viii)
Post-micturition leakage [1]: Complaint of a further involuntary passage of urine following the completion of micturition.
-
(ix)
Position-dependent micturition [1]: Complaint of having to take specific positions to be able to micturate spontaneously or to improve bladder emptying e.g., leaning forwards or backwards on the toilet seat or voiding in the semi-standing position.
-
(x)
Splinting to micturate: as above A (iv).
-
(xi)
Dysuria [1]: Complaint of burning or other discomfort during micturition. Discomfort may be intrinsic to the lower urinary tract or external (vulvar dysuria).
-
(xii)
(Urinary) retention [1]: Complaint of the inability to pass urine despite persistent effort.
-
(xiii)
Increased daytime urinary frequency [1]: Complaint that micturition occurs more frequently during waking hours than previously deemed normal by the woman.
-
(xiv)
Urgency [1]: Complaint of a sudden, compelling desire to pass urine which is difficult to defer.
E: Potential prolapse-related anorectal dysfunction symptoms [1, 8]
-
(i)
Constipation [8]: Complaint that bowel movements are infrequent and/or incomplete and/or there is a need for frequent straining or manual assistance to defecate2.
-
(ii)
Feeling of incomplete bowel evacuation [1, 8]: Complaint that the rectum does not feel empty after defecation and may be accompanied by a desire to defecate again.
-
(iii)
Straining to defecate [1, 8]: Complaint of the need to make an intensive effort (by abdominal straining or Valsalva) to either initiate, maintain or improve defecation.
-
(v)
Sensation of anorectal blockage [8]: Complaint suggestive of anorectal obstruction.
- (vi)
-
(vii)
Fecal (rectal) urgency [1, 8]: Complaint of a sudden compelling desire to defecate that is difficult to defer.
-
(viii)
Post-defecatory soiling (NEW): Soiling occurring after defecation.
F: Potential prolapse-related sexual dysfunction symptoms [1, 10, 17]
-
(i)
Dyspareunia: Complaint of persistent or recurrent pain or discomfort associated with attempted or complete vaginal penetration.
-
(ii)
Obstructed intercourse: Complaint that vaginal penetration is impeded. Possible causes include narrowing or a bulge.
-
(iii)
Vaginal laxity: Complaint of excessive vaginal looseness.
-
(iv)
Libido – loss or decrease: Complaint of loss or decrease of sexual desire
G: Other possible associated symptoms [1]
-
(i)
Urinary incontinence symptoms [1]: Urinary incontinence (symptom); stress (urinary) incontinence; urgency (urinary) incontinence; postural (urinary) incontinence; nocturnal enuresis; mixed (urinary) incontinence; continuous (urinary) incontinence; insensible (urinary) incontinence; coital (urinary) incontinence.
-
(ii)
Bladder storage symptoms [1]: nocturia; overactive bladder syndrome.
-
(iii)
Bladder sensory symptoms [1]: Increased bladder sensation; reduced bladder sensation; absent bladder sensation.
-
(iv)
Lower Urinary Tract Infection [1]: Urinary tract infection (UTI); recurrent urinary tract infections (UTIs); other related history.
H: More common POP-related symptoms:
Table 1 gives a consensus view of the authors of the more common POP-related symptoms
Signs
Sign: Any abnormality indicative of disease or a health problem, discoverable on examination of the patient; an objective indication of disease [16] or a health problem.
A: Signs of pelvic organ prolapse
All examinations for POP should be performed with the woman’s bladder empty (and if possible an empty rectum). An increasing bladder volume has been shown to restrict the degree of descent of the prolapse [18]. The choice of the woman’s position during examination, e.g., left lateral (Sims), supine, standing or lithotomy is that which can best demonstrate POP in that patient and which the woman can confirm as the maximal extent she has perceived e.g., by use of a mirror or digital palpation1. The degree of prolapse may be worse after a lengthy time in the upright position.
-
(i)
Pelvic organ prolapse (anatomical definition of the sign of POP) [1]: The descent of one or more of the anterior vaginal wall, posterior vaginal wall, the uterus (cervix) or the apex of the vagina (vaginal vault or cuff scar after hysterectomy). The presence of any such sign should be correlated with relevant POP symptoms [13, 19–21], i.e., patient report of maximal prolapse. More commonly, this correlation would occur at the level of the hymen or beyond [19–21].
-
(ii)
Pelvic organ prolapse – (POPQ) - (staging [1, 3, 4]):
-
Stage 0: No prolapse is demonstrated.
-
Stage I: Most distal portion of the prolapse is more than 1 cm above the level of the hymen.
-
Stage II: The most distal portion of the prolapse is situated between 1 cm above the hymen and 1 cm below the hymen3.. See also Appendix.
-
Stage III: The most distal portion of the prolapse is more than 1 cm beyond the plane of the hymen but everted at least 2 cm less than the total vaginal length.
-
Stage IV: Complete eversion or eversion at least within 2 cm of the total length of the lower genital tract is demonstrated.
-
-
(iii)
Uterine/ cervical prolapse: Observation of descent of the uterus or uterine cervix (Fig. 2).
Fig. 2 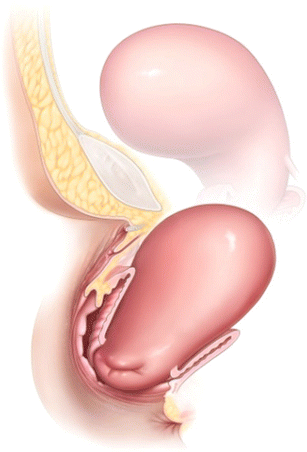
Uterine Prolapse
-
(iv)
Anterior vaginal wall (compartment) prolapse: Observation of descent of the anterior vaginal wall (compartment). Most commonly this might represent bladder prolapse (cystocele). Higher stage anterior vaginal wall prolapse will generally involve descent of uterus or vaginal vault (if uterus is absent). Occasionally, there might be an anterior enterocele (hernia of peritoneum and possibly abdominal contents), most commonly after prior reconstructive surgery (Fig. 3).
Fig. 3 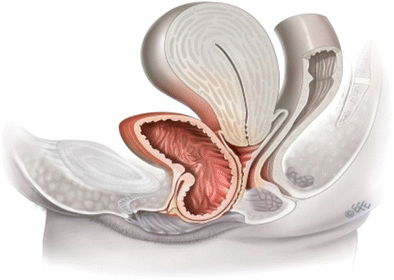
Anterior vaginal wall (compartment) prolapse
-
(v)
Posterior vaginal wall (compartment) prolapse: Observation of descent of the posterior vaginal wall. Commonly, this would represent rectal protrusion into the vagina (rectocele). Higher stage posterior vaginal wall prolapse after prior hysterectomy will generally involve some vaginal vault (cuff scar) descent and possible enterocele formation. Enterocele formation can also occur in the presence of an intact uterus (Fig. 4).
Fig. 4 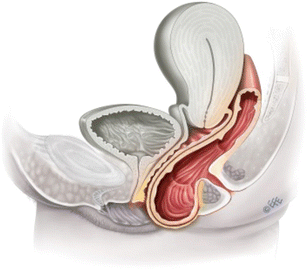
Posterior vaginal (compartment) wall prolapse
-
(vi)
Vaginal vault (cuff scar) prolapse: Observation of descent of the vaginal vault (cuff scar after hysterectomy) (Fig. 5).
Fig. 5 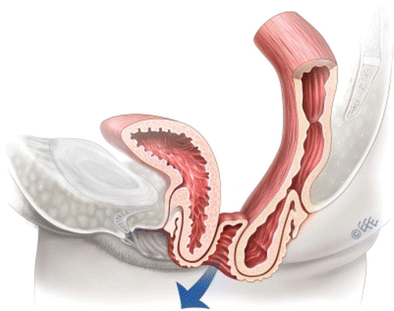
Vaginal vault prolapse




B: Clinical staging [4]
Each aspect of POP, uterine (cervical) prolapse, anterior vaginal wall (compartment), posterior vaginal wall (compartment), vaginal vault (cuff scar) prolapse can and should be subject to a clinical staging (Fig. 6).

shows prolapse staging [4] – 0, I, II, III, IV. (uterine – by the position of the leading edge of the cervix)
C: Supplementary physical examination techniques
-
(i)
Digital rectal-vaginal examination [4]: While the patient is straining and the prolapse is maximally developed. The aim is to try to differentiate between a high rectocele and an enterocele.
-
(ii)
Q-tip (urethral) testing [4]: Measurement of urethral axial mobility at rest and straining to assess degree of mobility.
D: Clinical assessment of associations of POP
-
(i)
Levator Defects / Trauma [22]: Per-vaginal palpation for levator injury/defect/ “avulsion”.
-
(ii)
Uterine retroversion [23, 24]: (Turning backward) The axis of the uterus is directed backwards towards the hollow of the sacrum, away from its anteverted position overlying the bladder. Cervix is noted in/ towards the anterior fornix with fundus perhaps palpable in the posterior fornix. Footnote 4
E: Other possible signs
-
(i)
Urinary incontinence signs [1]: Urinary incontinence; stress (urinary) incontinence; urgency (urinary) incontinence; extraurethral incontinence; stress incontinence on prolapse reduction (occult or latent stress incontinence)
-
(ii)
Other pelvic examinations/signs [1]: Vulvar examination; urethral inspection/palpation (urethral mucosal prolapse, urethral caruncle; urethral diverticulum); vaginal examination; bimanual pelvic examination; pelvic floor muscle function (normal pelvic floor muscles, overactive pelvic floor muscles, underactive pelvic floor muscles, non-functioning pelvic floor muscles); examination for levator (puborectalis) injury; perineal examination (perineal elevation, perineal descent); rectal examination (anal sphincter tone and strength, anal sphincter tear, fecal impaction present/absent, other rectal lesions, anal lesions, other perianal lesions), vaginal atrophy.
-
(iii)
Other relevant examinations/Signs [1]: Neurological signs, abdominal signs (bladder fullness/retention; abdominal masses or distension; scars from previous relevant surgery or trauma; renal tenderness or masses).
-
(iv)
Frequency volume chart / Bladder diary [1]
-
(v)
Pad testing [1]
Prolapse quantification
A: Pelvic organ prolapse quantification (POP-Q) [4]
-
(i)
Fixed Point of Reference. The hymen is the fixed point of reference used throughout the POP-Q system of quantitative prolapse description.
-
(ii)
Defined Points. The anatomic position of the six defined points (two on the anterior vaginal wall, two in the superior vagina, and two on the posterior vaginal wall) for measurement should be centimeters (cm) above or proximal to the hymen (negative number) or cm below or distal to the hymen (positive number) with the plane of the hymen being defined as zero (O). For example, a cervix that protruded 3 cm distal to the hymen would be + 3 cm. All points are measured on maximal straining (except total vaginal length).
-
(iii)
Anterior Vaginal Wall.
-
(a)
Point Aa. A point located in the midline of the anterior vaginal wall three (3) cm proximal to the external urethral meatus. By definition, the range of position of Point Aa relative to the hymen is −3 to +3 cm.
-
(b)
Point Ba. A point that represents the most distal (i.e., most dependent) position of any part of the upper anterior vaginal wall from the vaginal cuff or anterior vaginal fornix to Point Aa. By definition, Point Ba is at −3 cm in the absence of prolapse and would have a positive value equal to the position of the cuff (Point C) in women with total uterine prolapse or post-hysterectomy vaginal eversion.
-
(a)
-
(iv)
Superior Vagina. These points represent the most proximal locations of the normally positioned lower reproductive tract. The two superior sites are as follows:
-
(c)
Point C. A point that represents either the most distal (i.e., most dependent) edge of the cervix or the leading edge of the vaginal cuff (hysterectomy scar) after total hysterectomy.
-
(d)
Point D. A point that represents the location of the posterior fornix in a woman who still has a cervix. It is included as a point of measurement to differentiate suspensory failure of the uterosacral-cardinal ligament “complex” from cervical elongation. When the location of Point C is significantly more positive than the location of Point D, this is indicative of cervical elongation which may be symmetrical or eccentric. Point D is omitted in the absence of the cervix.
-
(c)
-
(v)
Posterior Vaginal Wall.
-
(e)
Point Ap. A point located in the midline of the posterior vaginal wall three (3) cm proximal to the hymen. By definition, the range of position of Point Ap relative to the hymen is − 3 to +3 cm.
-
(f)
Point Bp. A point that represents the most distal (i.e., most dependent) position of any part of the upper posterior vaginal wall from the vaginal cuff or posterior vaginal fornix to Point Ap. By definition, Point Bp is at −3 cm in the absence of prolapse and would have a positive value equal to the position of the cuff in a women with total post-hysterectomy vaginal eversion.
-
(e)
-
(vii)
Other Landmarks and Measurements.
-
(g)
The genital hiatus (GH) is measured from the middle of the external urethral meatus to the posterior margin of the hymen.
-
(h)
The total vaginal length (TVL) is the length of the vagina (cm) from posterior fornix to hymen when Point C or D is reduced to its full normal position. (See Fig. 41 - Appendix).
-
(i)
The perineal body (PB) is measured from the posterior margin of the hymen to the mid-anal opening.
-
(g)
-
(viii)
Recording Measurements: (NB: Intraoperative measurements with traction can be quite different from measurements made during Valsalva in clinic, both in regards to cervical location and the vaginal walls). Measurements directly after removing a vaginal pessary are unreliable and will tend to understage the degree of POP.
The position of Points Aa, Ba, Ap, Bp, C, and (if applicable) D with reference to the hymen should be measured (cm) and recorded (Figs. 7 and 8).

The six sites (Aa, Ba, C, D, Bp and Bp), the genital hiatus (gh), perineal body (pb) and total vaginal length (tvl) used cm above or proximal to the hymen (negative number) or cm below or distal to the hymen (positive number) with the plane of the hymen being defined as zero (0). Alternatively, a three by three grid can be used to organize concisely the measurements as noted in Fig. 8

Grid presentation of POP-Q measurements
B: Simplified POP-Q [25, 26]
This is based on the POP-Q with similar ordinal staging but with only four points measured instead of nine. There is no Stage 0; it is combined with Stage 1. It is undertaken in the dorsal lithotomy position with patient forcefully bearing down, performing Valsalva or coughing.
-
(i)
Four points used:
-
. Anterior vaginal segment: point Ba (estimated around 3 cm proximal to hymenal remnants).
-
. Posterior vaginal segment: point Bp (estimated around 3 cm proximal to hymenal remnants).
-
. Cervix point C
-
. Apex/posterior fornix: point D (non-hysterectomized); point C (hysterectomized) (Fig. 9)
Fig. 9 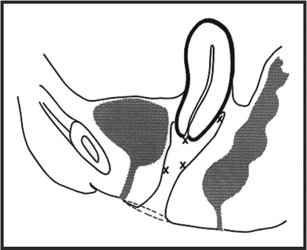
Simplified POP-Q
-

-
(ii)
Staging:
I, II, III, IV as for POP-Q above.
C: Additional available measurements awaiting further validation
These have been included as an Appendix after the References
-
(i):
Vaginal Anatomical Levels and Lengths.
-
(ii):
Perineal measurements.
-
(iii):
Vaginal measurements.
Investigations
Urodynamics [1]: Functional study of the lower urinary tract.
Clinical sequence of testing [1]: Urodynamic investigations generally involve a woman attending with a comfortably full bladder for free (no catheter) uroflowmetry and post void residual urine volume (PVR) measurement prior to filling and voiding (with catheter) cystometry.
A: Assessment of impact of prolapse on voiding function
POP can have a negative impact on voiding function, screening for which importantly involves a postvoid residual and ideally uroflowmetry. Voiding cystometry may clarify the cause of any voiding dysfunction.
-
(i)
Postvoid Residual [1–3]: Volume of urine left in the bladder at the completion of micturition. Conditions for PVR measurement:
PVR reading is erroneously elevated by delayed measurement due to additional urine production (1–14 mls/min). Ultrasonic techniques (transvaginal, translabial most accurately) allow immediate [27] (within 60 s of micturition) measurement and possible repeat measurement (Fig. 10). A short plastic female catheter provides the most effective bladder drainage for PVR measurement by catheterization.
Fig. 10 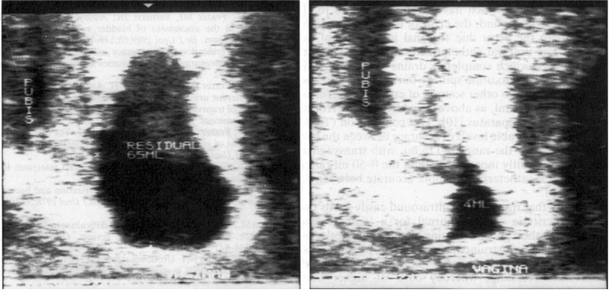
An image of postvoid residual of 65 ml by transvaginal ultrasound, reducing to 4 ml with a subsequent attempt at voiding
-
(ii)
Uroflowmetry [1–3]: Measurement of urine flow rates during micturition [16]
. Flow rate: Volume of urine expelled via the urethra per unit time. It is expressed in ml/sec.
. Voided volume (ml): Total volume of urine expelled via the urethra.
. Maximum (urine) flow rate (MUFR - ml/sec) - Qmax: Maximum measured value of the flow rate.
. Flow time (sec): The time over which measurable flow actually occurs.
. Average (urine) flow rate (AUFR- ml/sec) - Qave: Voided volume divided by the flow time (Fig. 11).
Fig. 11 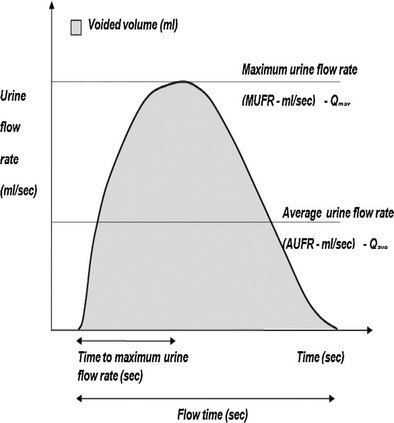
A schematic representation of urine flow over time


The dependence of urine flow rates on voided volume [28] makes it desirable to reference raw urine flow rate data to established normative data (Fig. 12).

-
(iii)
Pressure- Flow studies [1–3, 31]
Cystometry: Measurement of the pressure/volume relationship of the bladder during filling and/or pressure flow study during voiding. Higher voiding detrusor pressures and slower urine flow during voiding may point an element of bladder outflow obstruction [1–3, 32], though other patterns of pressure-flow data are possible (Fig. 13).
Fig. 13 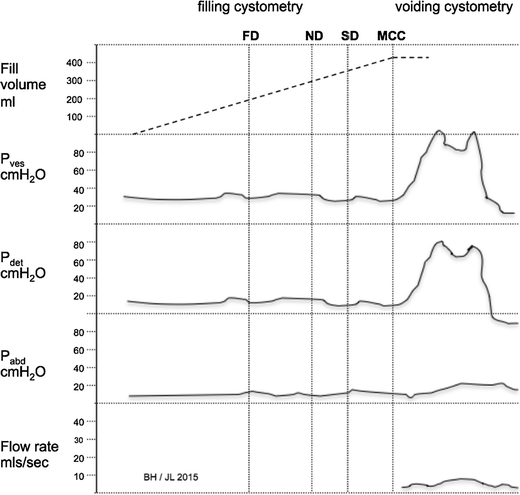
Filling and voiding cystometric trace, the latter part showing evidence of an element of bladder outflow obstruction. Normal bladder capacity, stable detrusor: no phasic activity seen. Voided with low urine flow rate and elevated detrusor pressure. Bladder outflow obstruction is thus demonstrated

B: Assessment of impact on prolapse on defecatory function
-
(i)
Ultrasound Assessment: See imaging section.
-
(ii)
Radiological Assessment: See imaging section.
C: Other urodynamic investigations for intercurrent diagnoses [1–3, 31]
-
(i)
Filling cystometry: The pressure/volume relationship of the bladder during filling can evaluate the presence of intercurrent diagnoses (ii–iv).
-
(ii)
Urodynamic stress incontinence [1]:
Involuntary leakage of urine during filling cystometry, associated with increased intra-abdominal pressure, in the absence of a detrusor contraction.
-
(iii)
Detrusor Overactivity [1]:
The occurrence of involuntary detrusor contractions during filling cystometry. These contractions, which may be spontaneous or provoked, produce a wave form on the cystometrogram, of variable duration and amplitude (Fig. 14).
Fig. 14 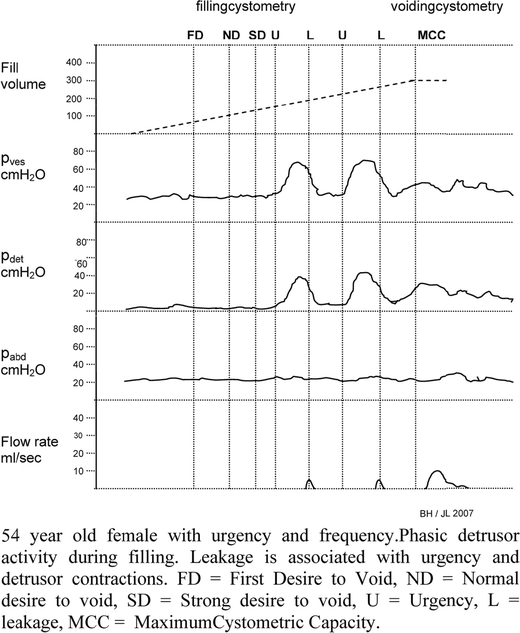
Cystometric trace showing detrusor overactivity [1]
-
(iv)
Bladder Oversensitivity [1]:
Increased perceived bladder sensation during bladder filling with: an early first desire to void; an early strong desire to void, which occurs at a low bladder volume; a low maximum cystometric bladder capacity. No abnormal increases in detrusor pressure are noted.
-
(v)
Detrusor underactivity [1], Footnote 5 and Acontractile detrusor [1], Footnote 6
Can also be diagnosed at voiding cystometry.

Prolapse imaging
Imaging may assist the clinical assessment of POP or intercurrent pelvic floor diagnoses. Use of any of the different imaging modalities is, however, entirely optional.
A: Prolapse-related ultrasound imaging – 2-D
-
(i)
Modalities
Transabdominal, perineal, introital and transvaginal ultrasound [1].
-
Transabdominal (T-A): curvilinear scanning applied to the abdomen.
-
Perineal: curved array probe applied to the perineum. This term incorporates transperineal and translabial ultrasound.
-
Introital: sector probe applied to the vaginal introitus.
-
Transvaginal (T-V): intravaginal curvilinear, linear array, or sector scanning.
-
-
(ii)
Clinical applications:
-
Bladder neck descent/mobility. The position of the bladder neck at rest and on Valsalva.
-
Urethral funnelling: i.e., opening of the proximal third of the urethra during coughing or on Valsalva.
-
Post void residual: Several formulas have been described in the literature to measure the bladder volume by ultrasound [33–35]. An early formula [(h × d × w) × 0.7] has been demonstrated to give reproducible results with a percentage error of 21 % [33] (see Fig. 15 for definitions of h,d,w).
Fig. 15 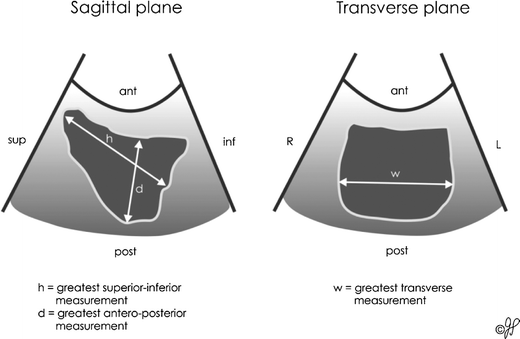
Ultrasound measurement of the bladder volume from Poston GJ et al. 1983 [33] (redrawn)
-
Bladder abnormalities: e.g., tumor, foreign body.
-
Urethral abnormality: e.g., diverticulum.
-
Intercurrent uterine and/or pelvic abnormality: dependent on probe range.
-
Postoperative findings: e.g., bladder neck position and mobility, position of meshes, tapes, or implants.
-
Descent of pelvic organs: visualization of descent of the bladder, uterine cervix, and rectum during coughing or on Valsalva.
-
Assessment of voluntary pelvic floor muscle contractility.
-
Pelvic floor/levator ani muscle defect (“avulsion”) and hiatal ballooning [36].
-
Ultrasound measurements of bladder and detrusor wall thickness, and ultrasound estimated bladder weight (UEBW) are potential noninvasive clinical tools for assessing the lower urinary tract. UEBW is higher in women with overactive bladder and detrusor overactivity [37, 38]. Footnote 7
-

Figures 16 and 17 show examples of 2-D introital ultrasound in patients with POP symptoms.

(right): 56 year old female with stage II cystocele and urodynamic stress incontinence. Left: at rest. Right: during valsalva. B Bladder, BB bladder base, U urethra, S symphysis pubis, arrow bladder neck during Valsalva, V vagina, R rectum. Arrow bladder neck during Valsalva with bladder neck funnelling as a sign of urethral incompetence

(above): 72 year old female with stage II rectocele. Measurement of rectocele (RC) width (1) and depth (2) during Valsalva. M muscularis of rectum
B: Prolapse-related ultrasound imaging – 3-D
-
(i)
Modalities: Endovaginal, transanal, and translabial/transperineal
-
Endovaginal ultrasound imaging may inadvertently compress tissues thus distorting the anatomy.
-
Transanal ultrasound approach requires an expensive and dedicated transducer, and it is a more uncomfortable and embarrassing test for the woman. Its most common clinical indication is the assessment of sphincter integrity following obstetric trauma.
-
Translabial/transperineal approach overcomes the limitations of endovaginal and transrectal techniques providing minimal pressure on local structures and it is least likely to alter surrounding anatomy.
-
-
(ii)
Evaluations:
The following pelvic floor abnormalities/ surgical sequelae can be evaluated:
-
(a)
Trauma (injury/damage) of the levator ani muscle (LAM).
-
(b)
Excessive distensibility of the puborectalis muscle and levator hiatus (“ballooning”).
-
(c)
Pathologies of the anterior vaginal compartment like urethral diverticula.
-
(d)
Bladder tumours or foreign bodies (sling, mesh, bulking agents).
-
Polypropylene meshes: highly echogenic and thus easily identified in the coronal and axial plane, unless they are obscured by vaginal prolapse.
-
Periurethral bulking agents, used as a continence procedure, can also be depicted with 3D pelvic floor ultrasound. Footnote 8
-
-
(a)
Figure 18 shows 3D ultrasound imaging of the pelvic floor anatomy.

(above): 3D ultrasound image of levator ani muscle of an asymptomatic nulliparous woman at rest. 3D ultrasound image of the pelvic floor at rest showing the anatomy and the reference plane of measurements. Left: sagittal view; PB pubic bone, U urethra, V vagina, ARA anorectal angle, white line: plane of minimal hiatal dimensions (plane of all measurements). Right: axial view, PB pubic bone, U urethra, V vagina, R rectum, PV pubovisceralis muscle; black line: antero-posterior diameter of the levator hiatus; white line: transverse diameter of the levator hiatus at the level of pubourethralis, white double- arrowed line: transverse diameter of the levator hiatus at the level of pubovaginalis
-
(iii)
3D ultrasound imaging of the female urethra
3D ultrasound imaging of the rhabdosphincter overcomes the limits of MRI and two-dimensional (2D) ultrasound imaging that incorrectly measure the urethral sphincter volume using mathematical formulas based upon assumptions that the shape of the urethra is similar to that of an ellipse. Since the urethral shape is neither elliptical nor spherical, but rather an atypical geometric shape, equations should not be used [39]. Footnote 9Figure 19 shows 3D ultrasound imaging of the urethral sphincter
Fig. 19 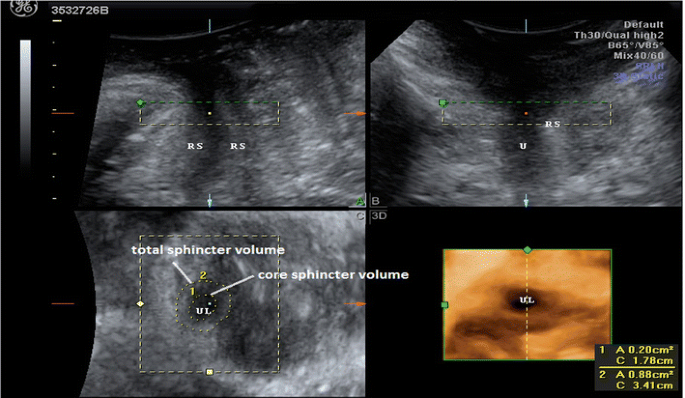
(above): 3D translabial image of the female urethra. The urethra lumen is shown clearly in the rendered volume image (bottom right). (U urethra, UL urethra lumen, RS rhabdosphincter)
-
(iv)
3D ultrasound imaging of the levator ani trauma
The presence of levator ani trauma has been postulated to be associated to an increased risk of pelvic organ prolapse [40]. This can be evaluated using a tomographic ultrasound imaging assessment of the levator ani muscles (Fig. 20).
Fig. 20 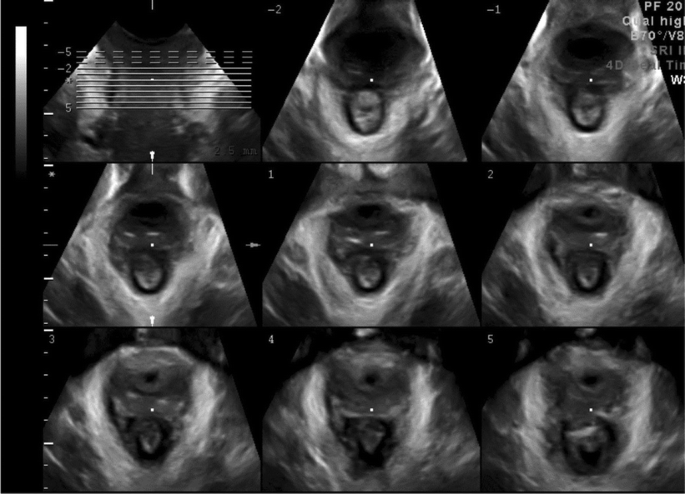
(above): Tomographic ultrasound imaging assessment of the levator ani muscles Intact LAM
-
(v)
3D ultrasound imaging of ballooning of the genital hiatus
The presence of ballooning of the genital hiatus ( = excessive distensibility of the levator hiatus) on Valsalva manoeuvre has also been associated to the severity of urogenital prolapse. An area of more than 25 cm2, 30 cm2, 35 cm2 and 40 cm2 has been defined as mild, moderate, marked and severe ballooning respectively (Fig. 21) [41].
Fig. 21 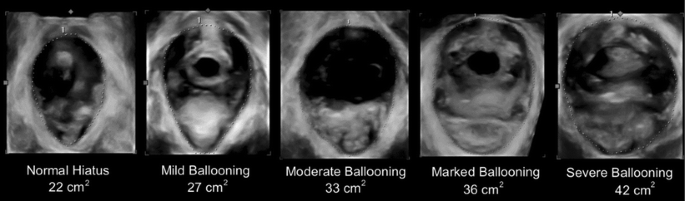
(above): Ballooning of the genital hiatus on Valsalva manoeuvre – levator defect



C: Magnetic resonance imaging (MRI) of the pelvic floor
Magnetic resonance imaging (MRI) allows the detection of ligamentous and muscular pelvic floor structures in fine detail. Although it does not use ionising radiation, it is a high cost technique. Static MRI relies on static sequences and high spatial resolution images, to delineate the passive and active elements of the pelvic organ support system. Most commonly, images are acquired in axial, sagittal and coronal planes.
MRI has been proposed to be a useful method for diagnosing and staging POP. Several lines and levels of reference have been described in the literature. The most commonly used ones are either a line drawn from the inferior margin of the pubis symphysis to the last coccygeal joint (pubococcygeal line—PCL) or a line extending caudally along the longitudinal axis of the symphysis pubis in the sagittal plane, noted as midpubic line (MPL) [42, 43] (Figs. 22 and 23).

(above): Sagittal MRI image of the pelvic floor obtained at rest in a 50-year-old normal volunteer woman. The H line is drawn from the inferior border of the pubic symphysis to the posterior wall of the rectum at the level of the anorectal junction. The M line is drawn perpendicularly from the PCL to the most posterior aspect of the H line. (PCL: pubococcygeal line, black arrow: bladder base, white arrow: vaginal vault, * : anorectal junction, from Colaiacomo MC [42] et al. 2009)

(above): Severe uterine prolapse in a 41-year-old woman. Sagittal function MRI image obtained during defaecation shows the uterus moving downward inside the vagina and the cervix exits the vaginal introitus (white arrow). H and M lines are abnormally elongated. Urethral funnelling without hypermobility (arrowhead) and severe posterior compartment descent (black arrow) are also noted (from Colaiacomo [42] et al. 2009)
Other applications of MRI are the assessment of the LAM morphology (size, thickness, volume) and detection of LAM injuries/ defects/ (“avulsion”) (Fig. 24) [44–46].

(above): Examples of grades of unilateral defects in the pubovisceral portion of the LAM in axial magnetic resonance images at the level of the mid urethra. The score for each side is indicated on the figure, and the black arrows indicate the location of the missing muscle (A. grade 1 defect; B. grade 2 defect; and C. grade 3 defect, from DeLancey. Levator Ani Impairment in Prolapse. Obstet Gynecol 2007)
D: Current possible measurements using MRI in urogynecology
-
(i)
Bladder neck and cervical descent / mobility:
-
Position of bladder neck and cervix at rest and on Valsalva
-
Pubo-coccygeal line: A line extending from the inferior border of the pubic symphysis to last coccygeal joint (pubococcygeal line—PCL) Bladder neck or cervical descent > 2 cm below this line with straining indicates weakness of the pelvic floor. If alternative landmarks are used in scientific papers they should be clearly described (Fig. 25).
Fig. 25 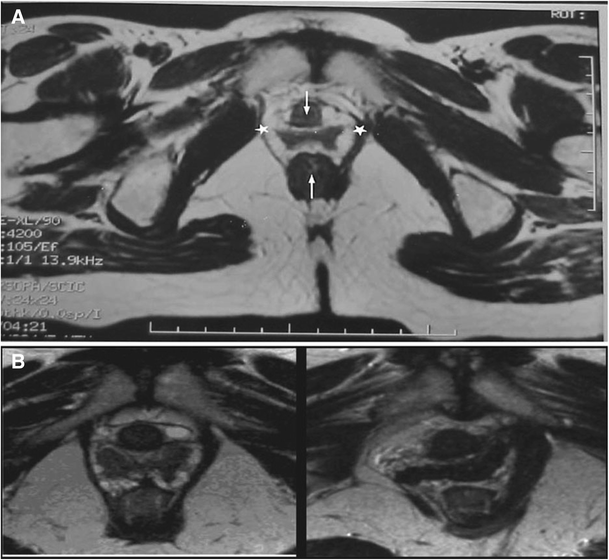
(above): shows a number of possible measurements using MRI imaging. a Axial T2-weighted image of the pelvic floor of a healthy nulliparous Caucasian woman showing measurement of the anteroposterior diameter of the genital hiatus between the arrows from midurethra to mid-anus at the level of the lower border of the pubic symphysis. Transverse diameter (width) of the levator hiatus was measured between the stars at the point of maximum extension of the levator muscles at the level of the urinary bladder and proximal urethra. Reproduced from Am J Obstet Gynecol with permission from the Publisher. b An example of a unilateral levator defect of the pubococcygeus muscle (right image) seen on MRI imaging. Reproduced with kind permission from Mr. Olubenga Adekanmi; image reviewed by Professor John DeLancey
-

E: Computed tomography (CT) of the pelvic floor
Computed tomography (CT) is not routinely recommended for imaging the pelvic floor mainly due to irradiation and poor soft tissue contrast. However multiplanar spiral CT may offer an accurate visualization of the pelvic floor soft and bony structures by reconstruction of axial images using 1 mm thick slices without gaps thus increasing the diagnostic accuracy of pelvic floor anatomical disorders (ie. LAM trauma) (Figs. 26 and 27).

(above): Computed tomography (CT) of the LAM. Axial view of CT multiplanar 3-dimensional data volume, with 1 mm slice thickness without gaps, showing an intact pubovisceral muscle arising from the body of the pubic bone and forming a sling around the rectum (U urethra, V vagina, R rectum, PM pubovisceral muscle, PR puborectalis muscle)

(above): Computed tomography (CT) of the LAM. Axial view of CT scan of a woman with bilateral injury of the pubovisceral muscle. Measurement of levator symphysis gap (LSG) is denoted bilaterally (U urethra, V vagina, R rectum, PM pubovisceral muscle)
F: Associated POP-related radiology [8]
Defecography demonstrates normal anatomy of the anorectum as well as disorders of rectal evacuation. With barium paste inserted rectally prior to defecation, measurement of the anorectal angle is allowed with evidence of the presence, size or emptying of any rectocele.
Enteroceles, rectal intusssusception and mucosal prolapse might be diagnosed as well as a spastic pelvic floor (anismus).
Diagnoses
This Report highlights the need to base diagnoses for female pelvic organ prolapse on the correlation between a woman’s symptoms, signs and any relevant diagnostic investigations.
A: Pelvic organ prolapse
Diagnosis by symptoms and clinical examination, assisted at times by any relevant imaging (i.e., clinically evident):
-
(i)
Uterine/ cervical prolapse: Clinically evident descent of the uterus or uterine cervix.
-
(ii)
Anterior vaginal wall (compartment) prolapse: Clinically evident descent of the anterior vaginal wall (compartment).
-
(iii)
Posterior vaginal wall (compartment) prolapse: Clinically evident descent of the posterior vaginal wall (compartment).
-
(iv)
Vaginal vault (cuff scar) prolapse: Clinically evident descent of the vaginal vault (cuff scar after hysterectomy).
Clinical staging (see Figs. 6, 28, 29 and 30) assists in description.

(above): Stage II Anterior vaginal wall (compartment) prolapse

(above): Stage III Uterine prolapse

(above): Stage IV Vaginal prolapse (complete eversion)
Figures 28, 29 and 30 : Different types and stages of pelvic organ prolapse.
B: Possible prolapse-related diagnoses
-
(i)
Voiding dysfunction: A diagnosis by symptoms and urodynamic investigations is defined as abnormally slow and/or incomplete micturition, based on abnormal slow urine flow rates and/or abnormally high post void residuals, ideally on repeated measurement to confirm abnormality. (Voiding cystometry can be required to determine the cause of the voiding dysfunction). Footnote 10
-
(ii)
Recurrent urinary tract infections (UTI): A diagnosis by clinical history assisted by the results of diagnostic tests involves the determination of the occurrence of at least three symptomatic and medically diagnosed urinary tract infections (UTI) over the previous 12 months. One possible POP-related cause is a chronically elevated postvoid residual.
-
(iii)
Defecatory dysfunction: A diagnosis by clinical history assisted, at times, by the results of diagnostic tests involving the confirmation of abnormal or difficult function in the initiation, passage or completion of defecation.
-
(iv)
Sexual dysfunction: A diagnosis by clinical history (including specific questionnaires) involving the confirmation of abnormal function and/or difficulty with sexual intercourse.
C: Intercurrent diagnoses
-
(i)
Urodynamic stress incontinence: Involuntary leakage of urine during filling cystometry, associated with increased intra- abdominal pressure, in the absence of a detrusor contraction. In the circumstances where this diagnosis is only made when the POP is reduced, the additional term “occult” is appropriate.
-
(ii)
Detrusor overactivity: The occurrence of involuntary detrusor contractions during filling cystometry.
-
(iii)
Bladder oversensitivity: Increased perceived bladder sensation during bladder filling with: an early first desire to void; an early strong desire to void, which occurs at a low bladder volume; a low maximum cystometric bladder capacity. No abnormal increases in detrusor pressure are noted.
-
(iv)
Detrusor underactivity [1, 5] and Acontractile detrusor [1, 6]
Conservative treatments
Conservative: restricted to non-surgical and non-pharmacological treatments.
A: Lifestyle interventions
Interventions that intentionally change the way a person lives in order to improve health status (e.g., weight loss and avoiding heavy lifting or coughing, e.g., by ceasing tobacco smoking), to avoid exacerbation of POP by decreasing intra-abdominal pressure.
B: Devices
Device: An object or instrument that has been invented/created for a particular purpose.
-
(i)
Pessary: A device that is inserted into the vagina to provide structural support to one or more of descending vaginal compartments, i.e., the uterus, anterior vaginal wall (and bladder), posterior vaginal wall (and rectum) and/or vaginal apex (with or without small intestine after a prior hysterectomy) [47].
Types of pessary: Vaginal pessaries can be broadly divided into two types: support pessaries (ring, ring with support, Gehrung, Hodge) and space filling pessaries (doughnut, gellhorn, cube, inflatable pessaries).
The most frequently used pessaries are listed below, as shown in Figs. 31 and 32 [47].

Pessaries (clockwise from top left) donut, cube, ring with central support, gellhorn

Shelf pessary
-
a.
Ring pessary with or without central support
-
b.
Gellhorn pessary; round solid pessary with a central stem
-
c.
Donut pessaryFootnote 11
-
d.
Cuboid pessaryFootnote 12
-
e.
Shelf pessary: Similar to a Gellhorn but asymmetric
C: Physical therapies [9]
Pelvic physiotherapy: Assessment, prevention and/or treatment of pelvic floor dysfunction, performed by a pelvic physiotherapist. The therapy aims at reducing POP symptoms and related bother as well as improvement of pelvic floor function. Pelvic physiotherapy covers many specialized therapies that can be used to train the pelvic floor: physical activity, cognitive behavioural therapy, bladder training, bowel habit training, muscle training (endurance, power), coordination training, biofeedback, and electrical muscle stimulation [9]. The role of continence nurses amongst other health professionals in performing some of these specialized therapies in acknowledged.
Other therapies: Refer to the terminology document of Bo et al [9].
Surgical treatments
A: General POP surgical terminology
-
(i)
Prosthesis [5]: A fabricated substitute to assist a damaged body part or to augment or stabilize a hypoplastic structure.
-
(ii)
Mesh [5]: A (prosthetic) network fabric or structure; open spaces or interstices between the strands of the net. The use of this term would be for POP surgery with synthetic materials.
-
(iii)
Mesh kit [5]: A set of articles or equipment utilized for POP surgery containing mesh with a system of trocars designed to achieve mesh fixation or allow mesh passage to or through specific areas within the pelvis.
-
(iv)
Implant [5]: A surgically inserted or embedded prosthesis or graft. (Explant: a surgically excised prosthesis or graft).
-
(v)
Tape (Sling) [5]: A flat strip of synthetic material. The use of this term would be for incontinence surgery with synthetic materials.
-
(vi)
Graft [5]: Any tissue or organ for transplantation. This term will be used to refer to biological materials inserted.
-
Autologous grafts: From patient’s own tissues e.g., rectus sheath or fascia lata. Allografts: From post-mortem tissue banks.
-
Xenografts: From other species e.g., modified porcine dermis, porcine small intestine and bovine pericardium.
-
Terminology for grafts has not been separated into the different applications for POP and continence surgery.
-
(vii)
Trocar [5]: A surgical instrument with either a pyramidal, conical or needle-type cutting or dissecting point.
-
(viii)
Tissue [6]: A collection of similar cells and the intercellular substances surrounding them.
-
(ix)
Native [6]: Pertaining to birth - “in situ autologous”.
B: Specific surgeries
The following classification of surgical procedure subtypes is proposed when describing specific surgeries. It is acknowledged that more complex cases may require two or more procedures in addition to other non-POP related surgical interventions. Each surgical procedure should be described with respect to site specificity and either as primary surgery or further surgery [7]. All surgical procedures are primarily divided by surgical approach as follows:
-
I.
Vaginal repairs:
-
(i)
Anterior vaginal wall repair with native tissue.
-
(ii)
Anterior vaginal wall repair with mesh or graft reinforcement.
-
(iii)
Posterior vaginal wall repair with native tissue.
-
(iv)
Posterior vaginal wall repair with mesh or graft reinforcement.
-
(v)
Vaginal vault repair involving uterus.
-
(vi)
Vaginal vault repair (post-hysterectomy).
-
(i)
-
II.
Abdominal repairs:
-
(i)
Abdominal Repair with Mesh or Graft.
-
(ii)
Abdominal Repair without Mesh or Graft.
-
(i)
-
III.
Obliterative Procedures:
-
(i)
Colpocleisis.
-
(ii)
Total colpectomy.
-
(i)
-
I:
Vaginal Repairs (colporrhaphy): (Greek: kolpo – vagina + raphe – suture)
-
(i)
Anterior vaginal wall repair with native tissue: Repair the vagina by excision and suturing of the edges of any defect. Native tissue repair may be further sub-classified depending on the type of associated fascial repair:
-
(a):
Midline fascial plication:. This represents perhaps the most common procedure currently performed for anterior wall prolapse [Fig. 33 below]. Footnote 13
Fig. 33 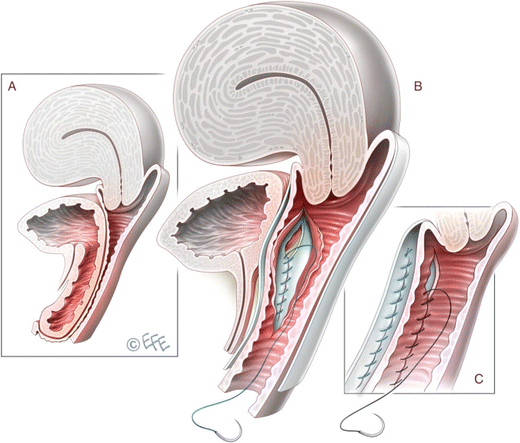
(right): Midline native tissue anterior vaginal repair
-
(b)
Site specific repair: Paravaginal – bilateral vaginal reattachment of the lateral edge of damaged fascia to the Arcus Tendineus Fasciae Pelvis (Alt: White line).
-
(c)
Other site specific repair: Transverse, distal, combined.
-
(d)
Anterior enterocele repair.
-
(a):
-
(ii)
Anterior Vaginal Wall Repair with mesh or graft reinforcement (a structural addition or inclusion used to give additional strength in function). It should be noted whether the graft is biologic, absorbable synthetic or permanent synthetic.
This may be further sub-classified into:
-
(a)
Mesh or graft placement without additional vault/uterine support with or without concurrent fascial plication.
-
(b)
Mesh or graft placement with additional vault/uterine support. This may be sud-divided into:
-
Transobturator mesh kit: Normally involves two needle passes through the obturator membrane bilaterally to retrieve and secure mesh arms through the area of the Arcus Tendineous Fasciae Pelvis (ATFP) and thus stabilize a central mesh support to the anterior vaginal wall.
-
Mesh kit with bilateral fixation to Sacrospinous Ligament [SSL]: Anterior vaginal wall mesh or graft with concurrent vault/ uterine suspension employing either bilateral iliococcygeal fixation or fixation to the SSL.
-
-
(a)
-
(iii)
Posterior vaginal wall repair with native tissue: Repair the vagina by excision and suturing of the edges of any defect. Native tissue repair may be further sub-classified depending on the type of associated fascial repair:
-
(a)
Midline fascial plication - This represents perhaps the commonest procedure currently performed for posterior wall prolapse and involves dissection under the full thickness of the vaginal epithelium followed by central plication of the pre-rectal fascia over the bulging rectum with excision of the ‘excess’ vaginal wall skin. [Fig. 34 below]
Fig. 34 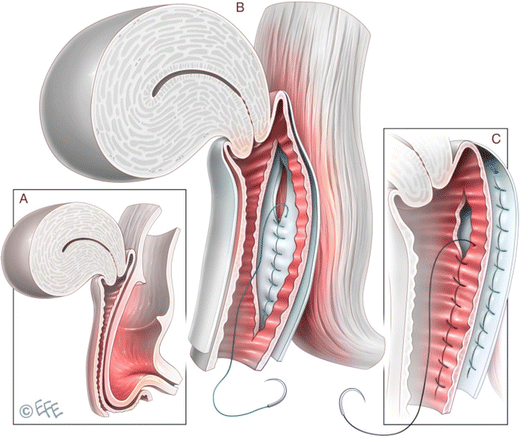
(right): Midline native tissue posterior vaginal repair
-
(b)
Site specific repair: Lateral (Uni- or Bilateral), Transverse (upper and/or lower), Combined
-
(c)
Closure and/or excision of enterocele vaginally with or without concurrent posterior wall repair.
-
(a)
-
(iv)
Posterior Vaginal Wall Repair with mesh or graft reinforcement (a structural addition or inclusion used to give additional strength in function. It should be noted whether the graft is biologic, absorbable synthetic or permanent synthetic.
This may be further sub-classified into:
-
(a)
Mesh or graft placement without additional vault/uterine support with or without concurrent fascial plication.
-
(b)
Mesh or graft placement with additional vault/uterine support. This may be sub-divided into:
-
(i)
Mesh kit with bilateral mesh fixation to the SSL.
-
(ii)
Mesh suspension kit with ischio-anal needle pass.
-
(iii)
Posterior vaginal wall mesh/graft with concurrent vault/uterine suspension employing either bilateral iliococcygeal fixation or fixation to the SSL.
-
(iv)
Transperineal mesh/graft insertion.
-
(i)
Concurrent surgery performed in addition to vaginal posterior wall repairs:
-
(a)
Perineal Repair (alternatives; Perineorrhaphy, Perineoplasty).
-
(b)
Levator ani muscle plication.
-
(c)
Repair/closure of enterocoele.
-
(d)
Anal sphincter repair.
-
(a)
-
(v):
Vaginal Vault Repairs (involving uterus)
-
(a)
Vaginal hysterectomy – removal of the uterus and cervix vaginally.
-
(b)
Vaginal hysterectomy with adjunctive McCall Culdoplasty – Culdoplasty sutures incorporate the uterosacral ligaments into the posterior vaginal vault to obliterate the cul-de-sac and support and suspend the vaginal apex after vaginal hysterectomy.
-
(c)
(Modified) Manchester Repair (Fothergill operation) – This procedure combines anterior vaginal wall repair with amputation of the cervix and uterosacral ligament suspension with or without concurrent vaginal posterior wall repair. Footnote 14
-
(d)
Sacrospinous hysteropexy - fixation of the uterus to the SSL. Variations of this technique to include:
-
(a)
Unilateral or bilateral procedure.
-
(b)
Anterior or posterior approach.
-
(c)
Permanent or absorbable suture and number of ‘bites’ taken.
-
(d)
Type of suture placement device employed.
-
(e)
Direct vision or with the use of a specific instrument (tactile feedback).
-
(a)
-
(e)
Laparoscopic assisted vaginal hysterectomy with or without concurrent laparoscopic uterosacral ligament plication.
-
(a)
-
(vi)
Vaginal Vault Repairs (Post-hysterectomy)
-
(a)
Sacrospinous colpopexy – Fixation of the vaginal vault to the SSL. Variations of this technique (as above a-e for sacrospinous hysteropexy) (Figs. 35 and 36).
Fig. 35 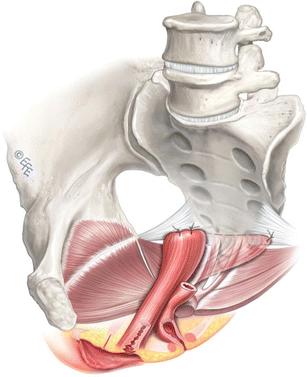
Sacrospinous colpopexy
Fig. 36 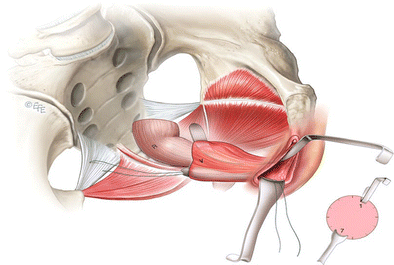
Suture placement around junction of medial third and lateral two-thirds of ligament assisted by retraction (Miya speculum 7 o’clock; narrow Deaver 1 o’clock; Yankauer sucker not shown)
-
(b)
Intraperitoneal uterosacral ligament (USL) vaginal vault fixation: This is usually associated with posterior wall fascial wall reconstruction and possible concurrent excision and closure of enterocele.
-
(c)
Extraperitoneal USL vaginal vault fixation: This is usually combined with posterior wall fascial reconstruction with or without enterocele closure and/or excision.
-
(d)
Mesh suspension kit with ischio-anal needle pass. The graft is fixed to the vault and elevation achieved when the upper graft arms are retrieved back through the levator ani muscle bilaterally.
-
(e)
Vaginal Trachelectomy for Cervical Stump Prolapse (previous subtotal hysterectomy) The cervical stump is removed in an identical fashion to the initial steps of a vaginal hysterectomy.
-
(a)
-
(i)




-
II
Abdominal Procedures
-
(i)
Abdominal Procedures with Mesh or GraftFootnote 15
-
(a)
Open / Laparoscopic / Robotic Sacrocolpopexy – Suspension of the vagina utilizing mesh or graft to the anterior longitudinal ligament usually at the level of the sacral promontory. (Fig. 37 below)
Fig. 37 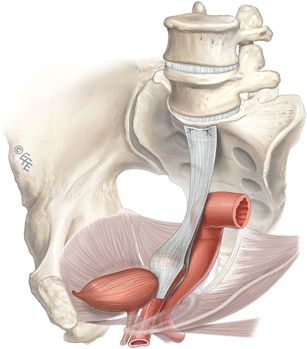
Sacrocolpopexy
-
(b)
Open / Laparoscopic / Robotic Sacrocervicocolpopexy – Suspension of the cervix (and usually vagina) utilizing mesh or graft to the anterior longitudinal ligament usually at the level of the sacral promontory. This procedure is commonly performed as an adjunct following subtotal hysterectomy for advanced utero-cervical prolapse.
-
(c)
Open / Laparoscopic / Open Sacrohysteropexy- suspension of the cervix (with or without additional vaginal attachment) utilizing mesh or graft to the anterior longitudinal ligament usually at the level of the sacral promontory. Sacrohysteropexy is performed for women who are keen to preserve their uterus.
-
(a)
-
(ii)
Abdominal Procedures without Mesh or Graft
-
(a)
Open / Laparoscopic / Robotic paravaginal repair – Extraperitoneal bilateral reattachment of the lateral edge of damaged fascia to the Arcus Tendineus Fasciae Pelvis (Alt: White line).
-
(b)
Laparoscopic / Robotic suture hysteropexy – The plicated uterosacral ligaments are resutured to the cervix.
-
(c)
Open / Laparoscopic / Robotic closure of enterocoele sac:
-
(a)
Moschowitz procedure- Concentric purse string suture(s) are placed around the cul-de-sac to include the posterior vaginal wall, pelvic side-walls and serosa of the sigmoid.
-
(b)
Halban procedure- Obliteration of the cul-de-sac by using successive sutures placed sagittally between the uterosacral ligaments.
-
(c)
Uterosacral ligament plication (Fig. 38 below) – transverse plication of the uterosacral ligaments to obliterate the cul-de-sac. Successive sutures are placed into the medial portion of one ligament, into the back wall of the vagina and into the medial border of the opposing ligament.
Fig. 38 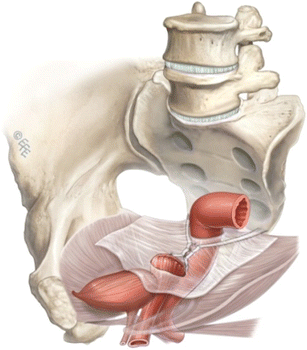
Uterosacral ligament plication
-
(a)
-
(d)
Open / Laparoscopic / Robotic Burch Colposuspension – Elevation or attachment of the upper paraurethral tissue adjacent to the bladder neck region to the iliopectineal ligament bilaterally. Although a recognized treatment for stress incontinence, this procedure will often correct associated anterior wall prolapse symptoms.
-
(a)
-
(i)


-
III:
Obliterative Procedures
-
(ii)
Colpocleisis: (Greek: kolpo + kleisis closure) – Operation for obliterating the lumen of the vagina. Footnote 16
-
(iii)
Total colpectomy: (Greek: kolpo + ektome excision): Total excision of the vagina in a woman with no uterus and vaginal eversion. Footnote 17
-
(ii)
C: Measuring outcome in POP surgeries [7]
As per IUGA-ICS Report on outcome measures for POP surgery [7], every study evaluating POP surgery should report.
-
(i)
Perioperative data: i.e., blood loss, operating time, length of hospital stay, return to normal activities and complications.
-
(ii)
Subjective (patient-reported) outcomes: At its simplest level this can be reported as the presence or absence of vaginal bulge. Patient satisfaction and quality of life can be measured by validated instruments that cover prolapse, urinary, bowel and sexual function.
-
(iii)
Objective outcomes: POP-Q measurement generally and should be tabulated with absolute values and percentages to allow other studies to compare results.
-
(iv)
Secondary outcomes (e.g., lower urinary tract symptoms, stress urinary incontinence or bowel and sexual dysfunction) in their studies whenever possible.
-
(v)
Surgery type and operated compartment:
-
(a)
Primary surgery: indicates the first procedure required for treating POP in any compartment.
-
(b)
Further surgery: provides a term for any subsequent procedure relating to primary surgery. Further surgery is subdivided into:
-
Primary surgery in a different (new) site/compartment.
-
Repeat surgery in the same site/compartment for POP symptom recurrence.
-
Surgery for complications e.g., mesh exposure, pain, infection or hemorrhage.
-
Surgery for non-POP-related conditions usually urinary or fecal incontinence.
-
-
(a)
D: Complications of POP surgeries [5, 6]
Complications related to POP native tissue repair and surgeries using prostheses/graft/mesh have been classified separately according to joint IUGA/ICS recommendation [5, 6]. The sorting system used in both documents utilizes specific category, time and site taxonomy together referred as CTS classification system. Classification is aided by on line calculators at either http://www.ics.org/complication or http://www.ics.org/ntcomplication.

This document has involved 14 rounds of full review, by co-authors, of an initial draft (Version 1) completed on November 30, 2014. Comments for each round of review were collated and debated as necessary in order to form a subsequent version. Live meetings on the document took place in Washington, Rio, Nice and Montreal.
Notes
In the era of advanced cellphone camera technology, a woman, at times, will bring photographic evidence of the prolapse at its worst. This can add to other clinical evidence, particularly if there is a discepancy between symptoms and signs.
The more formal classification of constipation is as follows:
Rome II diagnostic criteria for constipation:
• At least 12 weeks, which need not be consecutive, in the previous 12 months, of two or more of:
(i) Straining in > 1 in 4 defecations.
(ii) Lumpy or hard stools in > 1 in 4 defecations.
(iii) Sensation of incomplete evacuation in > 1 in 4 defecations.
(iv) Sensation of anorectal obstruction/ blockage in > 1 in 4 defecations.
(v) Manual manoeuvres to facilitate > 1 in 4 defecations (e.g.,: digital evacuation, support of the pelvic floor).
(vi) Less than 3 defecations per week.
• Loose stools are not present and there is insufficient evidence for IBS (irritable bowel syndrome)
A symptomatic-based subdivision of Stage II (see Appendix A) was overlooked at this time in favor of maintaining the current strictly anatomical definition of the “sign of POP”.
The axis of the retroverted uterus is parallel to that of the vaginal axis with less impediment to uterine (cervical) descent. In contrast, the anteverted uterus is perpendicular to the vaginal axis with impediment to descent by the posterior vaginal wall and behind that the rectum.
Detrusor underactivity: Detrusor contraction of reduced strength and/or duration, resulting in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span.
Acontractile detrusor: The detrusor cannot be observed to contract during urodynamic studies resulting in prolonged bladder emptying and/or a failure to achieve complete bladder emptying within a normal time span. The term “areflexia” has been used where there is a neurological cause but should be replaced by neurogenic acontractile detrusor.
Women with detrusor overactivity have a median UEBW of 48.0 g (95 % CI 46–51), with urodynamic stress incontinence a median UEBW of 30 g (95 % CI 29–31) and those who have associated detrusor overactivity and urodynamic stress incontinence have a median UEBW of 37.3 g (95 % CI 33–41) (p < 0.001) [37, 38]
Synthetic implant such as macroplastique, are hyperechogenic whereas collagen injections are hypoechoic and can be seen as spherical structures surrounding the bladder neck.
The importance of precise structural assessment of the urethral sphincter using multiple axial cross-sectional areas at set distances can assist the evaluation of women with stress urinary incontinence. It has been suggested that it may predict the severity of incontinence as well as the outcome of continence surgery since a weak sphincter will have a lower volume compared to a competent/continent urethral sphincter [39].
It is acknowledged this definition may not encompass cases of (i) symptoms of voiding dysfunction without abnormality of voiding parameters; (ii) abnormality of voiding parameters without symptoms of voiding dysfunction.
A more space occupying pessary.
A cuboid pessary does deliver ‘support’ by suction of the vaginal walls.
It was first described by Kelly in 1913 and involves dissection under the full thickness of the vaginal epithelium followed by central plication of the pubocervical fascia over the bulging bladder with excision of the ‘excess’ vaginal wall skin. The Kelly-Kennedy plication suture (Alt: bladder neck buttress) is an extrapolation of midline fascial plication involving placement of sutures under the proximal urethra and bladder neck to try and treat or prevent stress incontinence.
Its essential feature is suturing the cut cardinal/uterosacral ligament complex in front of the stump of the cervix hence pulling the cervix upwards and backwards, maintaining anteversion and creating anterior vaginal wall length.: This procedure can be performed intra- or extra-peritoneally. Concurrent McCall culdoplasty or vaginal vault suspension techniques may be employed dependant on the extent of prolapse [48].
Variations in technique for all abdominal mesh/graft procedures: (i) Type of mesh or graft used; (ii) Shape of mesh /graft- single piece,‘DIY’ two piece ‘Y’ mesh, Y mesh kit product; (iii) Points and length of attachment to vagina. (iv) Suture material employed / Metal stapling devices; (v) Peritoneal closure over mesh/graft.
This is usually performed in a woman with a uterus who is no longer sexually active. It can be performed in the absence of a uterus in a woman with vaginal eversion instead of total colpectomy. The Le Fort’s procedure involves denuding the vagina of skin both anteriorly and posteriorly, typically in a rectangular shape, avoiding the bladder neck and cervix. The cut edges are sewn together to achieve vaginal closure whilst leaving a bilateral epithelium-lined tunnel behind. The Labhardt procedure involves the removal of a 1 cm horse shoe shape of vaginal epithelium is removed over the posterior fourchette up to just under the urethra. By closing the incision and building up the perineum, an extremely high posterior repair almost closing the vagina is created.
The vagina is totally denuded of skin, typically in sections, whilst avoiding the bladder neck region. The prolapse is then reduced by a series of successive purse-string sutures and the epithelium at the entrance closed.
Mean length of Level II in women at posterior colporrhaphy found to be 5.0 cm [52]
The outer edge of the vestibule is known as Hart’s line (see white line in Fig. 39 with blue line demarcating anterior and posterior vestibule).
Mean length in women at posterior colporrhaphy was found to be 1.8 cm [52].
References
Haylen BT, Freeman RM, de Ridder D et al (2010) An International Urogynecological Association (IUGA)—International Continence Society (ICS) Joint report into the terminology for female pelvic floor dysfunction. Neurourol Urodyn 29:4–20, International Urogynecology J 2010;21:5–26
Abrams P, Blaivas JG, Stanton SL et al (1988) The standardisation of terminology of lower urinary tract function. Scand J Urol Nephrol Suppl 114:5–19
Abrams P, Cardozo L, Fall M et al (2002) The standardisation of terminology of lower urinary tract function. Report from the standardisation subcommittee of the International Continence Society. Neurourol Urodyn 21:167–178
Bump RC, Mattiasson A, Bo K et al (1996) The standardization of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol 175:10–11
Haylen BT, Freeman RM, Swift SE et al (2011) An International Urogynecological Association (IUGA) / International Continence Society (ICS) Joint Terminology and Classification of complications related directly to the insertion of prostheses (meshes, implants, tapes) and grafts in female pelvic floor surgery. Int Urogynecol J 22:3–15, Neurourology and Urodynamics 30(1):2–12
Haylen BT, Freeman RM, Lee J, et al (2012) An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint terminology and classification of the complications related to native tissue female pelvic floor surgery. Int Urogynecol 23:515–26. Neurourol Urodyn 31:406–14
Toozs-Hobson P, Freeman R, Barber M, et al (2012) An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint report on the terminology for reporting outcomes of surgical procedures for pelvic organ prolapse. Int Urogynecol 23:527–35. Neurourol Urodyn 31:415–26
Sultan A, Monga A, Haylen BT, et al (2015) An International Urogynecological Association (IUGA) / International Continence Society (ICS) Joint Report on the Terminology for Anorectal Dysfunction in Women (In Committee Review)
Bo K, Frawley H, Haylen BT, et al (2015) An International Urogynecological Association (IUGA) / International Continence Society (ICS) Joint report on the terminology for the conservative management of pelvic floor dysfunction. (In Committee Review)
Rogers R, Thakar R, Petri E, et al (2015) An International Urogynecological Association (IUGA)/International Continence Society (ICS) Joint report on the terminology for the sexual health in women with pelvic floor dysfunction. (In Committee Review)
Riss P, Dwyer PL (2014) The POP-Q classification system: looking back and looking forward. Int Urogynecol J 25:439–440
Bump RC (2014) The POP-Q system: two decades of progress and debate. Int Urogynecol J 25:441–443
Toozs-Hobson P, Swift S (2014) POP-Q stage 1 prolapse: is it time to alter our terminology? Int Urogynecol J 25:445–446
Harmanli O (2014) POP-Q 2. 0: its time has come. Int Urogynecol J 2014;25:447–449
(1995) Concise Oxford English Dictionary. 9th Edition. Oxford: Clarendon Press. p1438.
(2006) Stedman’s medical dictionary. 28th Edition. Lippincott William and Wilkins, Baltimore. p 1884
Rogers GR, Villarreal A, Kammerer-Doak D et al (2001) Sexual function in women with/without urinary incontinence and or pelvic organ prolapse. Int Urogynecol J 12:361–365
Yang A, Mostwin J, Genadry R et al (1993) Patterns of prolapse demonstrated with dynamic fastscan MRI; reassessment of conventional concepts of pelvic floor weaknesses. Neurourol Urodyn 12:310–311
Swift SE, Woodman P, O’Boyle A et al (2005) Pelvic Organ Support Study (POSST): the distribution, clinical definition and epidemiology of pelvic organ support defects. Am J Obstet Gynecol 192:795–806
Swift SE, Tate SB, Nichols J (2003) Correlation of symptomatology with degree of pelvic organ support in a general population of women: what is pelvic organ prolapse? Am J Obstet Gynecol 189:372–379
Barber MD, Brubaker L, Nygaard I et al (2009) Pelvic floor disorders network. Obstet Gynecol 114:600–609
Dietz HP (2007) Quantification of major morphological abnormalities of the levator ani. Ultrasound Obstet Gynecol 29:329–334
Haylen BT (2006) The retroverted uterus: Ignored to date but core to prolapse. Int Urogynecol J 17:555–558
Symmonds RE (1982) Relaxation of pelvic supports. In: Benson RC (ed) Current obstetrics and gynaecological diagnosis and treatment. Lange Medical Publications, Los Altos, pp 285–291 (chap 12)
Swift S, Morris S, McKinnie V et al (2006) Validation of a simplified technique for using the POPQ pelvic organ classification system. Int Urogynecol J 17:615–620
Parekh M, Swift S, Lemos N et al (2011) Multicentre inter-examiner trial of the validation of simplified POPQ system. Int Urogynecol J 22:645–650
Haylen BT, Lee J, Logan V et al (2008) Immediate postvoid residuals in women with symptoms of pelvic floor dysfunction: prevalences and associations. Obstet Gynecol 111:1305–1312
Fantl JA, Smith PJ, Schneider V et al (1982) Fluid weight uroflowmetry in women. Am J Obstet Gynecol 145:1017–1024
Haylen BT, Ashby D, Sutherst JR et al (1989) Maximum and average urine flow rates in normal male and female populations - the Liverpool nomograms. Br J Urol 64:30–38
Haylen BT, Parys BT, Ashby D et al (1990) Urine flow rates in male and female urodynamic patients compared with the Liverpool nomograms. Br J Urol 65:483–488
Schafer W, Abrams P, Liao L et al (2002) Good urodynamic practices: uroflowmetry, filling cystometry, and pressure-flow studies. Neurourol Urodyn 21:261–274
Groutz A, Blaivas JG, Chaikin DC (2000) Bladder outflow obstruction in women: definition and characteristics. Neurourol Urodyn 19:213–220
Poston GJ, Joseph AE, Riddle PR (1983) The accuracy of ultrasound in the measurement of changes in bladder volume. Br J Urol 55:361–363
Haylen BT, Frazer MI, Sutherst JR et al (1989) Transvaginal ultrasound in the assessment of bladder volumes in women. Br J Urol 63:152–154
Dietz HP, Velez D, Shek KL et al (2012) Determination of postvoid residuals by translabial ultrasound. Int Urogynecol J 23:1749–52
Pineda M, Shek K, Wong V et al (2013) Can hiatal ballooning be determined by two-dimensional translabial ultrasound? Aust N Z J Obstet Gynaecol 53:489–493. doi:10.1111/ajo.12111, Epub 2013 Aug 2
Bright E, Oelke M, Tubaro A et al (2010) Ultrasound estimated bladder weight and measurement of bladder wall thickness-useful noninvasive methods for assessing the lower urinary tract? J Urol 184:1847–1854. doi:10.1016/j.juro.2010.06.006
Panayi DC, Khullar V, Digesu GA et al (2009) Is ultrasound estimation of bladder weight a useful tool in the assessment of patients with lower urinary tract symptoms? Int Urogynecol J Pelvic Floor Dysfunct 12:1445–1449. doi:10.1007/s00192-009-0964-0
Digesu GA, Calandrini N, Derpapas A et al (2012) Intraobserver and interobserver reliability of the three-dimensional ultrasound imaging of female urethral sphincter using a translabial technique. Int Urogynecol J 8:1063–1068. doi:10.1007/s00192-012-1669-3, Epub 2012 Jan 21
Rodrigo N, Wong V, Shek KL et al (2014) The use of 3-dimensional ultrasound of the pelvic floor to predict recurrence risk after pelvic reconstructive surgery. Aust N Z J Obstet Gynaecol 3:206–211. doi:10.1111/ajo.12171, Epub 2014 Feb 18
Dietz HP, Shek C, De Leon J et al (2008) Ballooning of the levator hiatus. Ultrasound Obstet Gynecol 6:676–680. doi:10.1002/uog.5355
Colaiacomo MC et al (2009) Dynamic MR imaging of the pelvic floor: a pictorial review. Radiographics 29, e35
DeLancey JO, Morgan DM, Fenner DE et al (2007) Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstet Gynecol 109:295–302
Fielding JR (2002) Practical MRI, imaging of female pelvic floor weakness. RadioGraphics 22:295–304
Torricelli P, Pecchi A, Caruso-Lombardi A et al (2002) Magnetic resonance imaging in evaluating functional disorders of female pelvic floor. Radiol Med 103:488–500
Rizk DE, Czechowski J, Ekelund L (2004) Dynamic assessment of pelvic floor and bony pelvis morphologic condition with the use of magnetic resonance imaging in a multi- ethnic, nulliparous, and healthy female population. Am J Obstet Gynecol 191:83–89
Lamers BH, Broekman BM, Milani AL (2011) Pessary treatment for pelvic organ prolapse and health-related quality of life; a review. Int Urogynecol J 6:637–644
de Boer TA, Milani AL, Kluivers KB et al (2009) The effectiveness of surgical correction of uterine prolapse: cervical amputation with uterosacral ligament plication (modified Manchester) versus vaginal hysterectomy with high uterosacral ligament plication. Int Urogynecol J 20:1313–1315
DeLancey JO (1992) Anatomical aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol 166:117–124
Zemlyn S (1981) The length of the uterine cervix and its significance. J Clin Ultrasound 9:267–269
Vu D, Haylen BT, Tse K et al (2010) Surgical anatomy of the uterosacral ligament. Int Urogynecol J 21:1123–1128
Haylen BT, Kerr S, Naidoo S et al (2015) Posterior vaginal compartment repairs: where are the main anatomical defects? Neurourol Urodyn 34:S130–S131, Int Urogynecol J doi:10.1007/s00192-015-2874-7
Haylen BT, Avery D, Chiu T et al (2014) Posterior repair quantification (PR-Q) using key anatomical indicators (KAI). Int Urogynecol J 25(12):1665–1772, Neurourol Urodyn 2014;33:900–1
Haylen BT, Younis M, Naidoo S et al (2015) Perineorrhaphy quantitative assessment. Int Urogynecol J 26:539–544
Swenson CW, Simmen AM, Berger MB et al (2015) The long and short of it: anterior vaginal wall length before and after anterior repair. Int Urogynecol J 26:1035–1039
Acknowledgments
The assistance of Prof Steven Swift is gratefully acknowledged for the Simplified POP-Q section and other helpful input. Prof John DeLancey also contributed helpful input to “Prolapse quantification” and the Appendix. We thank our invited external reviewers Prof Steven Swift, Prof Mark Vierhout, Prof Michele Meschia, Prof Doug Tincello and Prof Don Wilson for their constructive contributions. We also thank those who submitted constructive comments following IUGA and ICS website presentation of Version 12: Dr Kiran Ashok, Prof Phil Toozs-Hobson, Dr Kamil Svabik. Further helpful comments were received at an open forum at ICS Montreal from Beth Shelly, Julia Herbert, Kari Bo and Joe Lee. The talents of medical illustrator, Levent Efe were crucial to the development of this document levent@leventefe.com.au.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
BT Haylen: No disclosures.
CF Maher: No disclosures.
MD Barber: No disclosures.
SFM Camargo: No disclosures.
V Dandolu: Research grant–Allegan, Consultant-Pfizer; A Digesu: Honorarium for lectures or sponsorship to cover travel expenses at Meetings from: Astellas, Pfizer, Allergan, AMS, Medtronic, Uroplasty.
HB Goldman: Consultant – Allergan, Medtronic, Uroplasty; Speaker – Astellas, Allergan, Medtronic, Uroplasty.
M Huser: No disclosures.
AL Milani: No disclosures.
PA Moran: Speaker & consultant: Astellas and Ethicon Women’s Health and Urology. Consultant: Boston Scientific.
GN Schaer: Advisor (in Switzerland) for Astellas, Novartis, Pfizer.
MIJ Withagen: Research Grant 2010–Ethicon Women’s Health & Urology.
Additional information
In the original version of this article, which can be found at 10.1007/s00192-015-2932-1, the color figures were mistakenly printed in black and white; the publisher apologizes for this error. The article is reproduced here in full with all figures rendered as the authors intended.
International Urogynecology Journal, Vol. 27, No. 2, 2016. Copyright 2016. This material is reproduced with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc., and the International Urogynecological Association.
This document is being published simultaneously in Neurourology and Urodynamics (NAU) and the International Urogynecology Journal (IUJ), the respective journals of the sponsoring organizations, the International Continence Society (ICS) and the International Urogynecological Association (IUGA) in the February 2016 issue of each journal.
Standardization and Terminology Committees IUGA - Bernard T. Haylen, Christopher F. Maher, Paul A. Moran, Gabriel. N. Schaer
Joint IUGA / ICS Working Group on Female POP Terminology - Bernard T. Haylen, Christopher F. Maher, Matthew D. Barber, Sérgio Camargo, Vani Dandolu, Alex Digesu, Howard B. Goldman, Martin Huser, Alfredo L. Milani, Paul A. Moran, Gabriel. N. Schaer, Mariëlla I. J. Withagen.
Published online in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/nau.22922.
Appendix - Concepts and available measurements awaiting further validation
Appendix - Concepts and available measurements awaiting further validation
A: Subdivision of Stage II POP-Q:
An optional subdivision of Stage II into IIa (−1 to hymen) and IIb (hymen to +1) was considered at length. Stage IIA would then be defined as −1 to 0 (so the hymen, that is 0, is included in stage IIA) and stage IIB (>0 to +1), meaning the dependent part of prolapse beyond the hymen but no further than +1. It was felt that this might reflect a clinical difference between the two subdivisions in terms of symptoms. That change was not made at this time in part to maintain the current strictly anatomical definition of the “sign of POP”.
B: Vaginal Anatomical Levels and Lengths:
-
(i)
Level I: Uterine cervix (if present) and/or upper 2.5 cm of vagina. Footnote Footnote 18
-
(ii)
Level II: Mid-vagina from distal end of Level I to hymen. Footnote 19
-
(iii)
Level III – Vaginal vestibule: Vaginal entrance (Latin: “vestibulum” = “a space at the entrance of a canal”) from hymenal ring to just below the clitoris anteriorly (anterior vestibule), labia minora laterally and anterior perineum posteriorly (posterior margin of vestibule) (Fig. 39)Footnote 20
Fig. 39 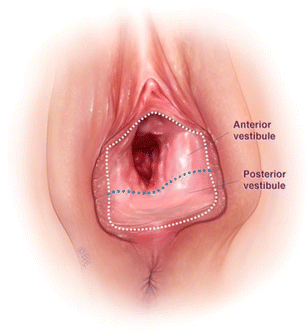
Anterior and posterior vestibule
-
(iv)
Posterior vestibule:Posterior hymenal ring to anterior perineum (posterior margin of vestibule) (Fig. 40)Footnote 21
-
(v)
Total vaginal length [4]: Posterior vaginal vault to hymen (cm), i.e., Levels I and II posteriorly.
-
(vi)
Total posterior vaginal length [52–54]: Posterior vaginal vault to posterior margin of vestibule (anterior perineum - cm), i.e., Levels I, II and III posteriorly.
-
(vii)
Anterior vaginal length: Anterior hymenal ring to the anterior vaginal vault (anterior cervicovaginal junction or anterior cuff post-hysterectomy) [55] (Fig. 41).


Posterior vestibule

Vaginal Levels (I to III) and Vaginal lengths (Anterior, Total, Total Posterior)
C: Additional available intraoperative measurements.
-
(i)
Perineal measurements:
-
(a,b)
Perineorrhaphy Width (PW) and Depth (PD) [54]: Width and depth of the excised perineum (Fig. 42)
Fig. 42 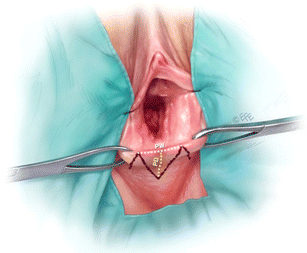
Perineorrhaphy width (PW) and perineorrhaphy depth (PD)
-
(c)
Perineal length (PL) [54]: Distance from posterior margin of vestibule to anterior anal verge (Fig. 43).
Fig. 43 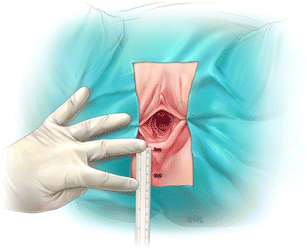
Perineal length
-
(d)
Mid-perineal thickness (MPT) [54]: Thickness (cm) of the mid-perineum in the midline (Fig. 44).
Fig. 44 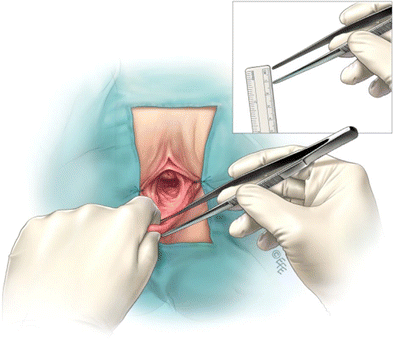
Mid-perineal thickness
-
(e)
Perineal Gap (PG) [52–54]: Thinned out medial area (cm) between Moynihan forceps placed bilaterally where the labia minora meet the perineum (Fig. 45).
Fig. 45 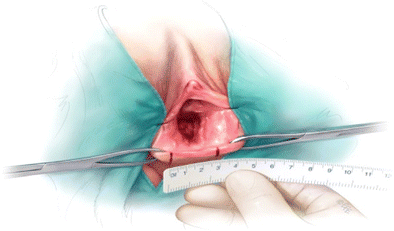
Perineal Gap
-
(f)
Perineorrhaphy Commencement Position (PCP): NEW Where in Level III, the perineorrhaphy is commenced, e.g., hymen, mid- vestibule, posterior margin of vestibule.
-
(a,b)
-
(ii)
Posterior vaginal measurements [53]:
-
(a)
Posterior Vaginal Vault Descent (PVVD [52, 53]: Descent of the posterior vaginal vault towards the perineal gap obtained by subtracting the inferiorly displaced vaginal vault and the anterior perineum (second figure) from the total posterior vaginal length (TPVL - first figure – posterior vaginal vault to anterior perineum). (Fig. 46 and Fig. 47)
-
(b)
Mid-Vaginal Laxity (MVL) (Undisplaced) [52, 53]: Laxity of the vaginal mucosa (anterior traction) midpoint in the vagina super- posteriorly and in the midline with the vaginal vault held in an undisplaced position (similar to that after vault fixation) (Fig. 48)
Fig. 46 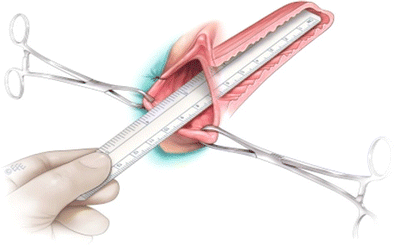
(above): Total posterior vaginal length (TPVL)
Fig. 47 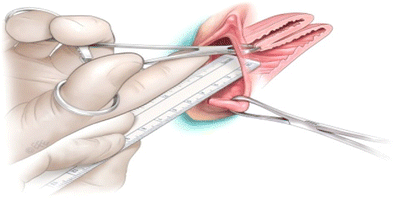
(above): Distance from vaginal vault (on traction) to anterior perineum. Posterior vaginal vault descent is the subtraction of this measurement from the TPVL
-
(c)
Recto-vaginal Fascial Laxity (RVFL) [52, 53]: Laxity of the rectovaginal fascia (anterior traction) midpoint in the vagina super- posteriorly (mucosa opened) and in the midline with the vaginal vault held in an undisplaced position (Figs. 49)
Fig. 48 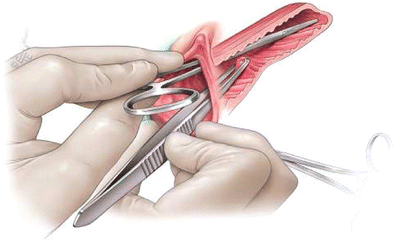
(above): Mid-vaginal laxity (vault undisplaced)
Fig. 49 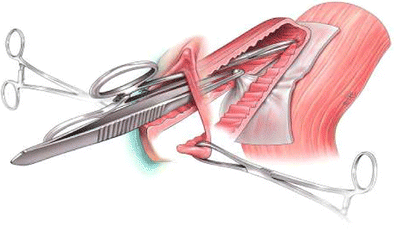
(above): Recto-vaginal fascial laxity
-
(a)








Rights and permissions
About this article

Cite this article
Haylen, B.T., Maher, C.F., Barber, M.D. et al. Erratum to: An International Urogynecological Association (IUGA) / International Continence Society (ICS) joint report on the terminology for female pelvic organ prolapse (POP). Int Urogynecol J 27, 655–684 (2016). https://doi.org/10.1007/s00192-016-3003-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-016-3003-y