
Abstract
Introduction and hypothesis
Suburethral sling procedures are a mainstay for the surgical treatment of stress urinary incontinence (SUI). The interaction between the sling and the host is fundamental for the success of the procedure. Patients affected by autoimmune disease present with an overactive immune system; this should theoretically increase rejection risk.
Methods
The data from 19 autoimmune patients affected by SUI were retrospectively collected. Primary outcome consisted of evaluating whether tape-related complications may occur more frequently. Secondary outcome measures were assessment of objective and subjective cure of SUI. Changes from baseline were analyzed using the Mann–Whitney and Fisher tests.
Results
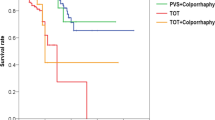
Success rate, evaluated at 12-month follow-up, was 89.5%. No tape erosion or urinary retention was observed; chronic pelvic pain and dyspareunia rates were 5.26% and 15.4%, respectively. One patient developed de novo urgency.
Conclusions
According to our experience, the suburethral sling is a safe procedure with low complication rates comparable to those reported in the literature.
Similar content being viewed by others


References
Ulmsten U, Petros P (1995) Intravaginal slingplasty (IVS): an ambulatory surgical procedure for treatment of female urinary incontinence. Scand J Urol Nephrol 29(1):75–82
Kaelin-Gambirasio I, Jacob S, Boulvain M, Dubuisson JB, Dällenbach P (2009) Complications associated with transobturator sling procedures: analysis of 233 consecutive cases with a 27 months follow-up. BMC Womens Health 9:28
Angioli R, Plotti F, Muzii L, Montera R, Panici PB, Zullo MA (2010) Tension-free vaginal tape versus transobturator suburethral tape: five-year follow-up results of a prospective, randomised trial. Eur Urol 58(5):671–677
Zullo MA, Plotti F, Calcagno M et al (2007) One-year follow-up of tension-free vaginal tape (TVT) and trans-obturator suburethral tape from inside to outside (TVT-O) for surgical treatment of female stress urinary incontinence: a prospective randomised trial. Eur Urol 51(5):1376–1382
Latthe PM, Singh P, Foon R, Toozs-Hobson P (2010) Two routes of transobturator tape procedures in stress urinary incontinence: a meta-analysis with direct and indirect comparison of randomized trials. BJU Int 106(1):68–76
Novara G, Artibani W, Barber MD et al (2010) Updated systematic review and meta-analysis of the comparative data on colposuspensions, pubovaginal slings, and midurethral tapes in the surgical treatment of female stress urinary incontinence. Eur Urol 58(2):218–238
Fairweather D (2007) Autoimmune disease: mechanisms. In: Encyclopedia of life sciences. Wiley, New York, pp 1–6
Auward W, Freeman RM, Swift S (2004) Is the pelvic organ prolapse quantification system (POPQ) being used? A survey of members of the International Continence Society (ICS) and the American Urogynecologic Society (AUGS). Int Urogynecol J Pelvic Floor Dysfunct 15:324–327
Abrams P, Andersson KE, Birder L et al (2010) Fourth International Consultation on Incontinence Recommendations of the International Scientific Committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn 29(1):213–240
Abrams P, Cardozo L, Fall M et al (2002) The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 21:167–178
De Leval J (2003) Novel surgical technique for the treatment of female stress urinary incontinence: transobturator vaginal tape inside-out. Eur Urol 44:724–730
Skala C, Renezeder K, Albrich S, Puhl A, Laterza RM, Naumann G, Koelbl H (2011) The IUGA/ICS classification of complications of prosthesis and graft insertion: a comparative experience in incontinence and prolapse surgery. Int Urogynecol J 22:1429–1435
Blaivas JG, Groutz A (2000) Bladder outlet obstruction nomogram for women with lower urinary tract symptomatology. Neurourol Urodyn 19:553–564
Tubaro A, Zattoni F, Prezioso D et al (2006) Italian validation of the International Consultation on Incontinence Questionnaires. BJU Int 97(1):101–108
Daneshgari F, Kong W, Swartz M (2008) Complications of mid urethral slings: important outcomes for future clinical trials. J Urol 180(5):1890–1897
Mistrangelo E, Mancuso S, Nadalini C, Lijoi D, Costantini S (2007) Rising use of synthetic mesh in transvaginal pelvic reconstructive surgery: a review of the risk of vaginal erosion. J Minim Invasive Gynecol 14(5):564–569, Review
Williams DF (1973) The response of the body environment to implants. In: Williams DF, Roaf R (eds) Implants in surgery. WB Saunders, Philadelphia, pp 203–297
Birch C (2005) The use of prosthetics in pelvic reconstructive surgery. Best Pract Res Clin Obstet Gynaecol 19(6):979–991
Jakus SM, Shapiro A, Hall CD (2008) Biologic and synthetic graft use in pelvic surgery: a review. Obstet Gynecol Surv 63(4):253–266
Von Theobald P (2011) Place of mesh in vaginal surgery, including its removal and revision. Best Pract Res Clin Obstet Gynaecol 25(2):197–203
del Rio ML, Lucas CL, Buhler L, Rayat G, Rodriguez-Barbosa JI (2010) HVEM/LIGHT/BTLA/CD160 cosignaling pathways as targets for immune regulation. J Leukoc Biol 87(2):223–235
Costantini E, Lazzeri M (2010) Elephants can remember. Eur Urol 58(5):678–679
Angioli R, Plotti F, Muzii L, Montera R, Benedetti Panici P, Zullo MA (2010) Reply from authors re: Elisabetta Costantini, Massimo Lazzeri. Elephants can remember. Eur Urol 58:678–679
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Angioli, R., Montera, R., Plotti, F. et al. Suburethral sling in autoimmune patients: complications, quality of life, and success rate. Int Urogynecol J 23, 453–457 (2012). https://doi.org/10.1007/s00192-011-1595-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-011-1595-9