
Abstract
Purpose
To evaluate the overall evidence of published health-economic evaluation studies on meniscus tear treatment.
Methods
Our systematic review focuses on health-economic evaluation studies of meniscus tear treatment interventions found in PubMed and Embase databases. A qualitative, descriptive approach was used to analyze the studies’ results and systematically report them following PRISMA guidelines. The health-economic evaluation method for each included study was categorized following one of the four approaches: partial economic evaluation (PEE), cost-effectiveness analysis (CEA), cost–benefit analysis (CBA), or cost-utility analysis (CUA). The quality of each included study was assessed using the Consensus on Health Economic Criteria (CHEC) list. Comparisons of input variables and outcomes were made, if applicable.
Results
Sixteen studies were included; of these, six studies performed PEE, seven studies CUA, two studies CEA, and one study combined CBA, CUA, and CEA. The following economic comparisons were analyzed and showed the respective comparative outcomes: (1) meniscus repair was more cost-effective than arthroscopic partial meniscectomy (meniscectomy) for reparable meniscus tear; (2) non-operative treatment or physical therapy was less costly than meniscectomy for degenerative meniscus tear; (3) physical therapy with delayed meniscectomy was more cost-effective than early meniscectomy for meniscus tear with knee osteoarthritis; (4) meniscectomy without physical therapy was less costly than meniscectomy with physical therapy; (5) meniscectomy was more cost-effective than either meniscus allograft transplantation or meniscus scaffold procedure; (6) the conventional arthroscopic instrument cost was lower than laser-assisted arthroscopy in meniscectomy procedures.
Conclusion
Results from this review suggest that meniscus repair is the most cost-effective intervention for reparable meniscus tears. Physical therapy followed by delayed meniscectomy is the most cost-effective intervention for degenerative meniscus tears. Meniscus scaffold should be avoided, especially when implemented on a large scale.
Level of evidence
Systematic review of level IV studies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Meniscus tears are the most prevalent and treated injuries in the knee joint, with a bimodal age distribution in young-active people and older people. Meniscus tear incidence is estimated at 60 per 100,000, although this number is likely underestimated [1]. Jarraya et al. found that over 75% of patients with symptomatic osteoarthritis have a meniscus tear [2]. Meniscus tear surgery is one of the most routinely performed orthopaedic procedures in the orthopedic field, with high annual costs [3]; therefore, early diagnosis and appropriate treatment for meniscus tears are increasingly crucial in current orthopedic research [1, 4].
Options to treat meniscus tears fall into two general categories: non-operative and operative management; the latter can be divided into three main methods: meniscectomy, either partial or total; meniscus repair; and meniscus transplantation, either meniscus scaffold or meniscus allograft transplantation [3]. Both host factors (e.g., age, co-morbidities, and compliance) and tear characteristics (e.g., location of tear/age/reducibility of tear) need to be considered before selecting the most appropriate treatment [5]. Evidence suggests that degenerative tears in older patients (age > 40) without mechanical symptoms can be effectively treated non-operatively with a structured physical therapy program as a first-line option. On the other hand, meniscus repair is more suitable for younger patients (age < 40) with peripheral reducible tears (e.g., nearer the capsular attachment) of the horizontal or longitudinal pattern and shows 80% success at two years [5, 6]. However, symptomatic tears not amenable to repair should be treated with meniscectomy, as meniscus function can still be preserved, especially when the peripheral meniscus rim is intact [5, 7].
As the concept of “value-based care” increasingly emerges, all aspects of health practice need to be re-evaluated to maintain health services’ affordability and sustainability. According to the Economist Intelligence Unit, value-based healthcare is “the creation and operation of a health system that explicitly prioritizes health outcomes which matter to patients relative to the cost of achieving this outcome” [8]. Hence, aggressive, preventive or curative interventions which are often costly but deliver outcomes with high effectiveness and efficiency are needed. Lowering the cost of treatments by sacrificing results is not an option in value-based healthcare [9]; therefore, understanding the cost drivers and high-value procedures within orthopedics is paramount if value-based health care is to be applied to this specialty. Specifically, the focus is to identify high-volume procedures with clear transparent choices and criteria and determine the value of these interventions.
A systematic review is important to look at the treatment of meniscus tears from a health-economic perspective. This study aimed to evaluate the evidence of published health-economic evaluation studies on meniscus treatment interventions. The health-economic studies associated with the procedure were identified, the data available were summarized, and the cost-effectiveness strategy among the procedures was determined.
Materials and methods
Overview and eligibility criteria for review
This systematic review was reported using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. It was registered in PROSPERO (Registration number: CRD42021262185). All economic studies published on PubMed and Embase databases were identified up to 30 April 2022. The following inclusion criteria were used: (1) cost analysis was performed on the meniscus tear’s treatment procedure; (2) based on either an economic model or a trial; and (3) clinical relevance to meniscus treatment. Analyses that did not report meniscus treatment-related cost values were excluded from the review. Studies issued as commentary, editorials, research protocols, and reviews, and studies not written in English were excluded.
Search method for identification of studies and data collection
A systematic search was conducted in two major electronic databases, PubMed and EMBASE. The references of the included studies were then reviewed to expand the search further and identify relevant publications. The search had no limitation for date of publication.
The search strategy was developed using the patient/population, intervention, comparison and outcomes (PICO) approach, which includes thesaurus and accessible terms related to or describing the condition and outcome. The PICO model was selected for its known relevance to defining clinical questions based on patients’ specific problems and the research question.
After reviewing the titles and abstracts, studies were included or excluded based on the inclusion criteria. Next, the full text was retrieved for further review for studies needing further inquiry into their inclusion status. Two authors (RD and MD) reviewed the full text of eligible studies for further data extraction. Review inconsistencies were resolved by joint review and consensus between reviewers.
Data synthesis and qualitative analysis of studies
All outcome variables reported in the included studies were extracted into the pre-specified data extraction form. Given the heterogeneity of the existing evidence, a qualitative, descriptive approach was used to assess the pooled results from the economic studies on meniscus treatment. The economic evaluation method of each included study was categorized into one of four approaches based on the availability of (1) comparison of two or more alternative interventions and (2) comparison of the costs and effects of the treatments in each study. The types of economic evaluations are partial economic evaluation (PEE), cost-effectiveness analysis (CEA), cost–benefit analysis (CBA), and cost-utility analysis (CUA) [10]. PEE measures disease cost without intervention comparison and does not relate costs to outcome. The costs of each treatment are analyzed straightforwardly in terms of monetary costs, assuming equal health outcomes for each intervention. CEA estimates the outcomes expressed in a natural health unit, such as number of patients with clinical improvement, cures, and life-years gained. The results of such comparisons may be stated either in terms of incremental cost per unit of effect. CBA measures and compares each intervention in terms of benefit and cost, all aspects expressed in monetary units. The results of CBA express the consequences of an intervention in monetary terms in order to facilitate comparison to program costs. CUA–often the preferred technique–measures and compares each intervention in terms of cost and utilities, indicating preferences for health outcomes using a generic measure of health gain, synthesized in cost per quality-adjusted life-year (QALY) [10, 11].
Regarding financial implications, comparisons were made for the following cost-related variables associated with the procedure: meniscus repair, arthroscopic partial meniscectomy (meniscectomy), physical therapy, non-operative treatment, meniscus allograft transplantation, meniscus scaffold, and other unique comparisons reported in a single study. Further, the type of meniscus tears behind these procedures was also classified as either reparable or irreparable meniscus tears. Costs included in this systematic review were converted to 2020 US dollars ($) using CCEMG-EPPI-Centre Cost Converter v.1.6 (accessible online at https://eppi.ioe.ac.uk/costconversion/), as suggested by Mastrigt et al. [11, 12].
A narrative data synthesis was performed by presenting all findings in summative form, including tables and figures. Primary outcomes were the average costs, effectiveness, and incremental cost-effectiveness ratio (ICER). Secondary outcome was the type of economic evaluation and the specificities of each study.
Quality assessment of studies
The CHEC list, which comprises 19 questions, was used to investigate the methodological quality of the economic studies by two independent reviewers (DI and AK). Each question is assigned either a “yes” or “no”. The two reviewers evaluated the papers and confirmed or disconfirmed compliance with each assessment question. Any disagreement was resolved by a joint review and consensus between reviewers. Each question in the CHEC list was rated with three possible answers: N = no, with no points; U = unclear, with half a point; and Y = yes, with one point. As the CHEC list does not define the summary scores specifically, we defined the score limits for the methodological quality of the studies; a total score ≥ 14.5 was considered a high-quality economic evaluation, a total score of 10–14 a moderate-quality economic evaluation, and a score < 10 a low-quality evaluation [8, 11, 13]. The agreement levels of interobserver assessment were determined by kappa value.
Statistical analyses were performed using SPSS Statistics version 26.0 (IBM).
Results
Study selection
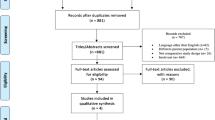
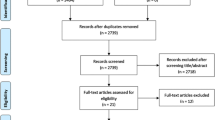
The search strategy identified 473 studies; after review of these initially selected studies, 16 were considered eligible for inclusion in our study (Fig. 1).

Study flow diagram as PRISMA guidelines[21].
General characteristics of included studies
The general characteristics of the included studies are presented in Table 1. A total of 16 studies were identified and included; six performed PEEs [7, 14,15,16,17,18], seven CUAs [6, 19,20,21,22,23,24], two CEA [25, 26], and one study performed a CUA, CEA, and CBA simultaneously [12]. Five studies compared meniscus repair vs meniscectomy [6, 7, 19, 20, 22], three studies compared costs of meniscectomy vs non-operative treatment [14, 17, 24], two studies compared physical therapy with delayed meniscectomy vs early meniscectomy [12, 21], two studies directly compared the costs of having vs not having physical therapy after a meniscectomy [15, 16], three studies investigated meniscus transplantation, and one study compared costs associated with conventional arthroscopic instruments vs laser-assisted treatment in meniscectomy [18].
The included studies varied geographically; 11 studies were conducted in the United States [6, 7, 14, 17,18,19,20,21,22, 25, 26], three studies in the Netherlands [12, 23, 24], and two in the United Kingdom [15, 16].
Methodological quality of the studies was assessed using the CHEC list and is displayed in Table 2. CHEC scores of the included studies ranged from 8 to 19. Agreement levels of interobserver assessment ranged from − 0.09 to 1 of kappa value. The entire agreement of each point of CHEC is reported in Appendix Table A 1–2.
Meniscus repair vs meniscectomy
Five studies compared meniscus repair vs meniscectomy. Two studies performed a direct comparison [6, 7], one study with additional non-operative treatment after medial meniscus root tears [19], one in the setting of ACL reconstruction [20], and another specifically involving red–red zone repair or meniscectomy [22]. In a large database study, Sochacki et al. [7] found that a meniscus repair costs more than a meniscectomy ($7,680 vs $5,871). However, the other four studies showed meniscus repair to be a more cost-effective treatment: Feeley et al. [6] compared meniscus repair vs meniscectomy (ICER $806/QALY vs $975/QALY), Faucett et al. [19] compared the treatment of meniscus root tear cases between meniscus repair, meniscectomy, and non-operation (ICER $3,483/QALY vs $5,127/QALY vs $3,969/QALY), Rogers et al. [22] compared isolated meniscus repair vs meniscectomy for the red–red zone (ICER $1,185/QALY vs $2,362/QALY), and Lester et al. [20] compared meniscus repair vs meniscectomy in the setting of anterior cruciate ligament reconstruction (ICER $1,056/QALY vs $1,533/QALY).
Meniscectomy vs non-operative treatment
Three studies compared meniscectomy vs non-operative treatment, two using PEE [14, 17] and one using CUA [24]. The two studies agreed that meniscectomy generated more cost than not operating ($3,993 vs $427, and $4,740 vs $1,862, respectively) [14, 17]. In addition, Rongen et al. [24] showed the result of ICER $3,574/QALY vs $2,740/QALY between meniscectomy and non-operative treatment.
Early meniscectomy vs physical therapy with delayed meniscectomy
Of the studies that compared early meniscectomy vs physical therapy with delayed meniscectomy, one examined patient with a non-obstructive meniscus tear [12]; one investigated patient with a meniscus tear in knee osteoarthritis [21]. Van de Graaf, et al. concluded that early meniscectomy was less cost-effective than physical therapy with delayed meniscectomy (ICER $83,047/QALY), with non-inferiority margins of 0.89 for QALY [12]; and Losina, et al. found that early meniscectomy was less cost-effective than physical therapy with optional delayed meniscectomy (ICER $116,320/QALY) [21].
Physical therapy vs non-physical therapy in a meniscectomy setting
Two PEE studies investigated physical therapy after meniscectomy [15, 16]. One stated that the mean cost per patient of providing outpatient physical therapy was $120 [15], the other compared the cost incurred by the group that had physical therapy with the group that did not ($3,906 vs $3,576) [16].
Meniscus transplantation
Two studies discussed meniscus allograft transplantation [25, 26], one demonstrating that it needs to be approximately one-third more effective in delaying osteoarthritis in previously meniscectomized knees to be cost-effective and stating that the mean costs of meniscus allograft transplantation are higher than those of non-operative treatment ($8,714 vs $3,061, respectively) [25]. The other study stated that meniscus allograft transplantation had been shown to reduce pain and improve function in patients with a discoid lateral meniscus tear and postponed total knee arthroplasty (TKA) rate for more years than meniscectomy, yet a meniscus allograft transplantation is more costly than meniscectomy ($16,007 vs $11,538, respectively) [26]. One study on CUA compared the cost-effectiveness of meniscus scaffold vs meniscectomy, showing that meniscus scaffold was less cost-effective than meniscectomy both for a lifetime (ICER $73,445/QALY) and for a five-year period (ICER $401,492/QALY) [23].
Unique comparison data
One PPE study discussing conventional instruments vs laser-assisted meniscectomy concluded that conventional meniscectomy was recommended for routine intervention as the cost was lower ($1,796 vs $2,503, respectively) [18]. The results of the included studies are presented in Table 3.
Discussion
This study evaluates the evidence of published health-economic evaluation studies on meniscus tear treatment. The most important finding of the present study was cost-effectiveness of meniscus tear treatment depending on type of meniscus tear. Meniscus repair is more cost-effective for reparable meniscus tears, while physical therapy with delayed meniscectomy is more cost-effective for irreparable and degenerative meniscus tears.
This review showed that meniscus repair instead of meniscectomy; non-operative treatment instead of meniscectomy; physical therapy with delayed meniscectomy instead of early meniscectomy; meniscectomy without physical therapy vs meniscectomy with physical therapy; meniscectomy instead of meniscus allograft transplantation; and conventional instrument instead of laser-assisted meniscectomy gave more value. It was also concluded that meniscus scaffold should be avoided, especially when implemented on a large scale.
Surgery is usually recommended for most meniscus tears except those causing minor symptoms in less active patients, and is urgently recommended for locked knees [1, 5, 27, 28]. Treatment aims to preserve as much functional meniscal tissue as possible. Clinical symptoms caused by meniscus tears should also be addressed. However, room for discussion is still wide open about whether surgery’s increased benefits outweigh the higher costs. Non-operative treatment may be offered for a meniscus tear in less mobile, passive, and less demanding patients, as symptoms may be minimal or uncommon [1, 5, 29].
It is possible to classify meniscus tears into two broad categories: reparable and irreparable tears. Reparable tears present in young patients with horizontal tears in the vascular zone plus longitudinal and radial tears, and are usually traumatic cases [6, 30]. Tears are irreparable if they occur in the avascular zone or complex pattern, and most are degenerative cases [2, 29]. Repairs are generally performed in mild arthrosis (KL grade ≤ 2), mild varus alignment, and a chondral injury grade ≤ grade 2. Poor prognosis is predicted in repairs done on severe cartilage degeneration and severe varus malalignment [31]. The studies included in this systematic review followed the standard procedure of treatments for meniscus tears and lesions, choosing repairs for reparable tears and meniscectomy and/or other non-operative modalities for irreparable tears. This needed to be emphasized, as it proved that the included studies did not discard the importance of accurate and evidence-based treatment choice, although the focus was on cost-effectiveness.
Sochacki et al. concluded that meniscus repair costs more than meniscectomy [7]. This is most likely due to initial differences in implant cost [19, 32]. Day-of-surgery costs are also higher in meniscus repair than in meniscectomy [19]. Meniscus repair becomes more cost-effective after 10 and 30 years of operation because the rate of knee osteoarthritis and TKA is lower [6]. Physical therapy followed by delayed meniscectomy is the treatment of choice for degenerative meniscus tear. Losina et al. [21] and van de Graaf et al. [12] investigated degenerative types of meniscus tear for presence of knee osteoarthritis and horizontal-type tear with complex degenerative meniscus, respectively. Both papers showed that physical therapy followed by delayed meniscectomy is more cost-effective than early meniscectomy for degenerative meniscus tear.
The results found in this study regarding traumatic and degenerative meniscus lesions are in line with those of a previous study describing meniscus repair as the preferred strategy for traumatic meniscus injury, and physical therapy followed by delayed meniscectomy as the preferred intervention for degenerative meniscus tear [29, 30]. The findings from the health-economic perspective could support the development of recommendations for clinical practice guidelines in this field, explicitly considering health-economic evidence such as costs and cost-effectiveness.
The previous health-economic review describing meniscus scaffold and meniscal allograft as likely more effective than meniscectomy for medial meniscus injury and lateral discoid meniscus tear is being in line with the findings [26, 33]. This is because meniscus scaffold interventions are more effective in reducing pain and improving function, and postpone the rate of TKA for longer than meniscectomy [23, 26]. However, using the standard threshold of $50,000 as a basis of the cost-effectiveness strategy, meniscus scaffold is a less cost-effective strategy than meniscectomy, with an ICER of $73,445/QALY for a lifetime and an ICER of $401,492/QALY for five-year time horizon [23].
This review included either model-based or trial-based studies, both of which are mutually supportive and provide prominent evidence for health-economic assessments. A trial-based study presents direct and exact evidence in a particular field. However, because the time horizon of such a study is limited, its results should be used with reservations. A longer time horizon is favored for a health-economic assessment, which could be resynthesized by a model-based study. Although guided by trial-based studies in small populations, clinicians, payers, and regulators are likely to use a model-based study to sharpen their decision-making.
The risk of bias needs to be assessed in the included studies, as bias can overestimate or underestimate the actual intervention effect. There are available tools to evaluate the risk of bias in economic evaluations. Mastrigt et al. explain that the CHEC checklist is a preferred option for appraising trial-based and model-based economic evaluations [10]. Most of the included studies had an appropriate score on the CHEC list, so the findings of this systematic review can be considered low in risk of bias while providing valuable information to support health technology assessment in this field.
This review has some limitations. First, the heterogeneity and diversity of all included data could result in bias. Although the majority of included studies were considered of moderate-to-high-quality economic evaluation, the CHEC score of all included data is broad, ranging from 8 to 19. The level of agreement from − 0.09 to 1.0 of the kappa values showed some disagreement between the reviewers. The kappa value is frequently used to access interrater reliability and represents the extent to which the data collected in the study are correct representations of the variable measured [34]. However, the judgments about the acceptable kappa value for health research should be contingent on the researcher’s perception of what is relevant to the field of research. In this review we still included studies with a low kappa value, thanks to the critical evidence of the included studies [34].
Next, indirect cost assessment in health care is typically measured through loss of productivity and absenteeism. However, only six out of 16 included studies assessed this cost element, so we could not provide indirect cost reporting. Accordingly, recommendations on a more cost-effective treatment based on meniscus type could not be accurately formulated as there were various types of menisci and pre-existing knee conditions. Plus, only a limited number of studies were investigated. Some topics were discussed in a single economic analysis, including using a meniscus scaffold to treat meniscus tears. Hence, strong recommendations on this topic cannot be provided. Last, the results of studies conducted in the USA and Europe could not be transferable to other countries due to the diversity of healthcare systems. Studies in other regions are, therefore, needed.
This study showed the most cost-effective treatment for some types of meniscus tears. Clinicians can use the findings of this review in their day-to-day practice by considering each patient’s type of meniscus tear in their decision-making process. Although costs alone should not drive decision-making, but cost-effectiveness should be taken into consideration during discussion of treatment options with the patient.
Conclusion
Various meniscus treatment modalities are available for the treating surgeon to choose, broadly classified into meniscus repair, meniscectomy, non-operative approach with or without physical therapy, and meniscus transplantation. Results from this review conclude that meniscus repair is the most cost-effective intervention for reparable meniscus tears, while the physical therapy with delayed meniscectomy is the preferred strategy for degenerative meniscus tears. At the same time, meniscus scaffold should be avoided, especially when implemented on a large scale.
Data availability
The authors declare that the data supporting the findings of this study are available within the article [and its supplementary information files].
References
Bhan K (2020) Meniscal tears: current understanding, diagnosis, and management. Cureus 12(6):e8590
Jarraya M, Roemer FW, Englund M (2017) Meniscus morphology: does tear type matter? A narrative review with focus on relevance for osteoarthritis research. Semin Arthritis Rheum 46(5):552–561
Doral MN, Bilge O, Huri G, Turhan E, Verdonk R (2018) Modern treatment of meniscal tears. EFORT Open Rev. 3(5):260–268
Zhou T, Xu Y, Xu W (2020) Emerging research trends and foci of studies on the meniscus: a bibliometric analysis. J Orthop Surg (Hong Kong) 28(3):2309499020947286
Mordecai SC, Al-Hadithy N, Ware HE, Gupte CM (2014) Treatment of meniscal tears: An evidence based approach. World J Orthop. 5(3):233–241
Feeley BT, Liu S, Garner AM, Zhang AL, Pietzsch JB (2016) The cost-effectiveness of meniscal repair versus partial meniscectomy: A model-based projection for the United States. Knee 23(4):674–680
Sochacki KR, Varshneya K, Calcei JG (2020) Comparing meniscectomy and meniscal repair: a matched cohort analysis utilizing a national insurance database. Am J Sports Med 48(10):2353–2359
Purba AKR, Setiawan D, Bathoorn E, Postma MJ, Dik JH, Friedrich AW (2018) Prevention of surgical site infections: a systematic review of cost analyses in the use of prophylactic antibiotics. Front Pharmacol 18(9):776
Putera I (2017) Redefining health: implication for value-based healthcare reform. Cureus 9(3):e1067
van Mastrigt GA, Hiligsmann M, Arts JJ (2016) How to prepare a systematic review of economic evaluations for informing evidence-based healthcare decisions: a five-step approach (part 1/3). Expert Rev Pharmacoecon Outcomes Res 16(6):689–704
Deviandri R, van der Veen HC, Lubis AMT, van den Akker-Scheek I, Postma MJ (2022) Cost-effectiveness of ACL treatment is dependent on age and activity level: a systematic review. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-022-07087-z
van de Graaf VA, van Dongen JM, Willigenburg NW (2020) How do the costs of physical therapy and arthroscopic partial meniscectomy compare? A trial-based economic evaluation of two treatments in patients with meniscal tears alongside the ESCAPE study. Br J Sports Med 54(9):538–545
Afzali T, Fangel MV, Vestergaard AS, Rathleff MS, Ehlers LH, Jensen MB (2018) Cost-effectiveness of treatments for non-osteoarthritic knee pain conditions: a systematic review. PLoS ONE 13(12):e0209240
Barnds B, Morris B, Mullen S, Schroeppel JP, Tarakemeh A, Vopat BG (2019) Increased rates of knee arthroplasty and cost of patients with meniscal tears treated with arthroscopic partial meniscectomy versus non-operative management. Knee Surg Sports Traumatol Arthrosc 27(7):2316–2321
Forster DP, Frost CE (1982) Cost-effectiveness study of outpatient physiotherapy after medial meniscectomy. Br Med J 284(6314):485–487
Goodwin PC, Ratcliffe J, Morrissey MC (2005) Physiotherapy after arthroscopic partial meniscectomy surgery: an assessment of costs to the National Health Service, patients, and society. Int J Technol Assess Health Care 21(4):452–458
Hershman EB, Jarvis JL, Mick T, Dushaj K, Elsner JJ (2020) Direct treatment cost outcomes among patients with medial meniscus deficiency: results from a 24 month surveillance study. Curr Med Res Opin 36(3):427–437
Yakin DE, Rogers VP (1999) Conventional instrument vs. laser-assisted arthroscopic meniscectomy. Laser Surg Med 25(5):435–437
Faucett SC, Geisler BP, Chahla J et al (2019) Meniscus root repair vs meniscectomy or nonoperative management to prevent knee osteoarthritis after medial meniscus root tears: clinical and economic effectiveness. Am J Sports Med 47(3):762–769
Lester JD, Gorbaty JD, Odum SM, Rogers ME, Fleischli JE (2018) The cost-effectiveness of meniscal repair versus partial meniscectomy in the setting of anterior cruciate ligament reconstruction. Arthroscopy 34(9):2614–2620
Losina E, Dervan EE, Paltiel AD (2015) Defining the value of future research to identify the preferred treatment of meniscal tear in the presence of knee osteoarthritis. PLoS ONE 10(6):e0130256
Rogers M, Dart S, Odum S, Fleischli J (2019) A Cost-effectiveness analysis of isolated meniscal repair versus partial meniscectomy for red-red zone, vertical meniscal tears in the young adult. Arthroscopy 35(12):3280–3286
Rongen JJ, Govers TM, Buma P, Grutters JP, Hannink G (2016) Societal and economic effect of meniscus scaffold procedures for irreparable meniscus injuries. Am J Sports Med 44(7):1724–1734
Rongen JJ, Govers TM, Buma P, Rovers MM, Hannink G (2018) Arthroscopic meniscectomy for degenerative meniscal tears reduces knee pain but is not cost-effective in a routine health care setting: a multi-center longitudinal observational study using data from the osteoarthritis initiative. Osteoarthritis Cartil 26(2):184–194
Bendich I, Rubenstein W, Mustafa Diab M, Feeley B (2018) Evaluating meniscus allograft transplant using a cost-effectiveness threshold analysis. Knee 25(6):1171–1180
Ramme AJ, Strauss EJ, Jazrawi L, Gold HT (2016) Cost effectiveness of meniscal allograft for torn discoid lateral meniscus in young women. Phys Sportsmed 44(3):278–282
Zhang T, Jauregui JJ, Foster M et al (2021) Outcomes of partial meniscectomy in obese patients: a systematic review and meta-analysis. Cartilage 13(1_suppl):216S-227S
Zhou ML, Haley CC (2021) Meniscal ramp lesions and root tears: a review of the current literature. Sports Med Arthrosc Rev 29(3):158–167
Beaufils P, Becker R, Kopf S et al (2017) Surgical management of degenerative meniscus lesions: the 2016 ESSKA meniscus consensus. Knee Surg Sports Traumatol Arthrosc 25(2):335–346
Kopf S, Beaufils P, Hirschmann MT et al (2020) Management of traumatic meniscus tears: the 2019 ESSKA meniscus consensus. Knee Surg Sports Traumatol Arthrosc 28(4):1177–1194
Lee JK, Jung M, Yang JH (2020) Repair versus nonrepair of medial meniscus posterior root tear: a systematic review of patients’ selection criteria, including clinical and radiographic outcomes. Medicine (Baltimore) 99(10):e19499
Deviandri R, van der Veen HC, Lubis AMT, Utoyo GA, van den Akker-Scheek I, Postma MJ (2022) Burden and cost of anterior cruciate ligament reconstruction and reimbursement of its treatment in a developing country: an observational study in Indonesia. Clinicoecon Outcomes Res 17(14):479–486
Yow BG, Donohue M, Tennent DJ (2021) Meniscal allograft transplantation. Sports Med Arthrosc Rev 29(3):168–172
McHugh ML (2012) Interrater reliability: the kappa statistic. Biochem Med (Zagreb) 22(3):276–282
Higgins J, Thomas J (2019) Cochrane Handbook for Systematic Reviews of Interventions. Available from www.handbook.cochrane.org. Accessed Jan 2022
Azar MF, Beaty HJ (2021) Campbell’s operative orthopaedics, 14th edn. Canale ST, Daugherty KC
Otsuki S, Ikeda K, Tanaka K, Okamoto Y, Sezaki S, Neo M (2022) Implantation of novel meniscus scaffold for irreparable meniscal tear. Arthrosc Tech 11(5):e775–e779
Page MJ, McKenzie JE, Bossuyt PM (2020) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 29(372):n71
Acknowledgements
We extend our gratitude to the librarians of the UMCG Central Medical Library, especially to Mrs. K.I (Karin) Sijtsma for her facilitation in this research.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
RD have made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data, and drafting the manuscript. MD, AL, DI, AK, and MJP have made substantial contributions to conception and design, analysis and interpretation of data, revising the manuscript, and final approval.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest related to this study.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Deviandri, R., Daulay, M.C., Iskandar, D. et al. Health-economic evaluation of meniscus tear treatments: a systematic review. Knee Surg Sports Traumatol Arthrosc 31, 3582–3593 (2023). https://doi.org/10.1007/s00167-022-07278-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-022-07278-8