
Abstract
Purpose
Graft diameter ≥ 8 mm reduces the risk of failure after anterior cruciate ligament reconstruction (ALCR) with hamstring tendon autograft. Pre-operative measurement of gracilis (GT) and semitendinosus (ST) cross-sectional area using MRI has been utilized but the optimal location for measurement is unknown. The main purpose of this study was to examine the cross-sectional areas of GT + ST at different locations and develop a model to predict whether a doubled hamstring graft of GT + ST will be of sufficient cross-sectional area for ACLR.
Methods
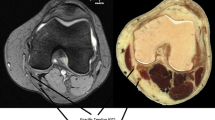
A retrospective review was performed of 154 patients who underwent primary ACLR using doubled hamstring autograft. Cross-sectional area measurements of GT + ST on pre-operative MRI axial images were made at three locations: medial epicondyle (ME), tibiofemoral joint line (TJL), and tibial physeal scar (TPS) and calculated the correlation of intra-operative graft size for each location using the Pearson’s correlation coefficient. A receiver operating characteristic (ROC) established a threshold that would predict graft diameter ≥ 8 mm.
Results
Measurement of GT + ST at the ME had a stronger correlation (r = 0.389) to intra-operative graft diameter than measurements at the TJL (r = 0.256) or TPS (r = 0.240). The ROC indicated good predictive value for hamstring graft diameter ≥ 8 mm based on MRI measurement at the ME with the optimal threshold with the highest sensitivity and specificity as 18 mm2.
Conclusion
Cross-sectional area measurement of GT + ST at the ME correlated most closely to intra-operative diameter of a doubled hamstring autograft compared to measurements at the TJL or the TPS. As graft diameter < 8 mm is correlated with higher failure rates of ACL surgery, the ability to pre-operatively predict graft diameter is clinically useful.
Level of evidence
Level III, prognostic study.



Similar content being viewed by others


Abbreviations
- ACL:
-
Anterior cruciate ligament
- GT:
-
Gracilis tendon
- ST:
-
Semitendinosus
- MRI:
-
Magnetic resonance imaging
- CT:
-
Computed tomography
- BMI:
-
Body mass index
- ROC:
-
Receiver operating characteristic
- AUC:
-
Area under the curve
- ANOVA:
-
Analysis of variance
- ICC:
-
Intraclass correlation coefficient (ICC)
References
Agarwal S, de Sa D, Peterson DC, Parmar D, Simunovic N, Ogilvie R et al (2018) Can preoperative magnetic resonance Imaging predict intraoperative autograft size for anterior cruciate ligament reconstruction? A systematic review. J Knee Surg. https://doi.org/10.1055/s-0038-1666830
Astur DDC, Novaretti JV, Liggieri AC, Janovsky C, Nicolini AP, Cohen M (2018) Ultrasonography for evaluation of hamstring tendon diameter: is it possible to predict the size of the graft? Rev Bras Ortop 53:404–409
Beyzadeoglu T, Akgun U, Tasdelen N, Karahan M (2012) Prediction of semitendinosus and gracilis autograft sizes for ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 20:1293–1297
Bickel BA, Fowler TT, Mowbray JG, Adler B, Klingele K, Phillips G (2008) Preoperative magnetic resonance imaging cross-sectional area for the measurement of hamstring autograft diameter for reconstruction of the adolescent anterior cruciate ligament. Arthroscopy 24:1336–1341
Conte EJ, Hyatt AE, Gatt CJ Jr, Dhawan A (2014) Hamstring autograft size can be predicted and is a potential risk factor for anterior cruciate ligament reconstruction failure. Arthroscopy 30:882–890
Erickson BJ, Harris JD, Fillingham YA, Frank RM, Bush-Joseph CA, Bach BR Jr et al (2014) Anterior cruciate ligament reconstruction practice patterns by NFL and NCAA football team physicians. Arthroscopy 30:731–738
Erquicia JI, Gelber PE, Doreste JL, Pelfort X, Abat F, Monllau JC (2013) How to improve the prediction of quadrupled semitendinosus and gracilis autograft sizes with magnetic resonance imaging and ultrasonography. Am J Sports Med 41:1857–1863
Goyal S, Matias N, Pandey V, Acharya K (2016) Are pre-operative anthropometric parameters helpful in predicting length and thickness of quadrupled hamstring graft for ACL reconstruction in adults? A prospective study and literature review. Int Orthop 40:173–181
Grawe BM, Williams PN, Burge A, Voigt M, Altchek DW, Hannafin JA et al (2016) Anterior cruciate ligament reconstruction with autologous hamstring: can preoperative magnetic resonance imaging accurately predict graft diameter? Orthop J Sports Med 4:2325967116646360
Koo TK, Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 15:155–163
Mariscalco MW, Flanigan DC, Mitchell J, Pedroza AD, Jones MH, Andrish JT et al (2013) The influence of hamstring autograft size on patient-reported outcomes and risk of revision after anterior cruciate ligament reconstruction: a Multicenter Orthopaedic Outcomes Network (MOON) Cohort Study. Arthroscopy 29:1948–1953
Mehran N, Moutzouros VB, Bedi A (2015) A review of current graft options for anterior cruciate ligament reconstruction. JBJS Rev 3:11
Momaya AM, Beicker C, Siffri P, Kissenberth MJ, Backes J, Bailey L et al (2018) Preoperative Ultrasonography is unreliable in predicting hamstring tendon graft diameter for ACL reconstruction. Orthop J Sports Med 6:2325967117746146
Serino J, Murray R, Argintar EH (2017) Use of magnetic resonance imaging to predict quadrupled semitendinosus graft diameter in all-inside anterior cruciate ligament reconstruction. Orthopedics 40:e617–e622
Steiger JH (1980) Tests for comparing elements of a correlation matrix. Psychol Bull 87:245–251
Wernecke G, Harris IA, Houang MT, Seeto BG, Chen DB, MacDessi SJ (2011) Using magnetic resonance imaging to predict adequate graft diameters for autologous hamstring double-bundle anterior cruciate ligament reconstruction. Arthroscopy 27:1055–1059
Yasumoto M, Deie M, Sunagawa T, Adachi N, Kobayashi K, Ochi M (2006) Predictive value of preoperative 3-dimensional computer tomography measurement of semitendinosus tendon harvested for anterior cruciate ligament reconstruction. Arthroscopy 22:259–264
Zakko P, van Eck CF, Guenther D, Irrgang JJ, Fu FH (2017) Can we predict the size of frequently used autografts in ACL reconstruction? Knee Surg Sports Traumatol Arthrosc 25:3704–3710
Zeng C, Gao SG, Li H, Yang T, Luo W, Li YS et al (2016) Autograft versus allograft in anterior cruciate ligament reconstruction: a meta-analysis of randomized controlled trials and systematic review of overlapping systematic reviews. Arthroscopy 32:153–163 e118
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
All authors (1) have made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data, (2)have been involved in drafting the manuscript or revising it critically for important intellectual content, (3) have given final approval of the version to be published, (4) agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
The study was approved by the institutional review board (IRB) at our institution.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hodges, C.T., Shelton, T.J., Bateni, C.P. et al. The medial epicondyle of the distal femur is the optimal location for MRI measurement of semitendinosus and gracilis tendon cross-sectional area. Knee Surg Sports Traumatol Arthrosc 27, 3498–3504 (2019). https://doi.org/10.1007/s00167-019-05421-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05421-6