
Abstract
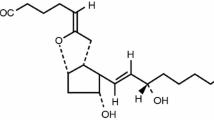
Objective: To study the effects of 6 h inhalation of aerosolized prostacyclin (PGI2) on platelet function.¶Design: In a prospective, double-blind, randomized study, 28 patients scheduled for elective cardiac surgery requiring cardiopulmonary bypass (CPB), received either 0.9 % sodium chloride (n = 8), PGI2 5 μg × ml–1 (n = 10) or PGI2 10 μg × ml–1 (n = 10) as an aerosol for 6 h postoperatively.¶Setting: Cardiothoracic intensive care unit at a university hospital.¶Interventions: All patients were studied immediately after surgery during mechanical ventilation and sedation. The PGI2 solutions or saline were administered with a jet nebulizer.¶Measurements and results: Bleeding time and chest tube drainage were measured. Blood samples for platelet aggregation, thrombelastography (TEG) and analysis of coagulation parameters and the stable prostacyclin metabolite 6-keto-PGF1α were obtained immediately before inhalation and after 2, 4 and 6 h of inhalation. After 6 h of PGI2 inhalation, regardless of administered dose, there was a lower rate of platelet aggregation and a lower maximal increase in light transmission in response to adenosine diphosphate (ADP) than in the control group. The TEG variable reaction time (R) was prolonged after 4 and 6 h of inhalation in the PGI2 group receiving 10 μg × ml–1. There were no differences between groups with respect to bleeding time and chest tube drainage or any of the other variables examined.¶Conclusion: Inhalation of PGI2 for 6 h in patients after cardiac surgery is associated with impaired platelet aggregation detected by in vitro techniques, with no in vivo signs of platelet dysfunction.
Article PDF
Similar content being viewed by others

Author information
Authors and Affiliations
Additional information
Received: 11 May 1999/Final revision received: 1 December 1999/Accepted: 10 December 1999
Rights and permissions
About this article
Cite this article
Haraldson, Å., Kieler-Jensen, N., Wadenvik, H. et al. Inhaled prostacyclin and platelet function after cardiac surgery and cardiopulmonary bypass. Intensive Care Med 26, 188–194 (2000). https://doi.org/10.1007/s001340050044
Issue Date:
DOI: https://doi.org/10.1007/s001340050044