
Abstract
Purpose
To examine the association of intravenous iodinated contrast material administration with the subsequent development of post-contrast AKI (PC-AKI), emergent dialysis, and short-term mortality using a propensity score-adjusted analysis of a cohort of intensive care unit (ICU) patients who underwent CT examination.
Methods
All ICU patients at our institution who received a contrast-enhanced (contrast group) or unenhanced (noncontrast group) CT scan from January 2006 to December 2014 were identified. Patients were subdivided into pre-CT eGFR > 45 and eGFR ≤ 45 subsets and separately underwent propensity score analysis. Rates of KDIGO-defined AKI, dialysis, and mortality were compared between contrast and noncontrast groups. Separate analyses of eGFR ≥ 60, 30–59, and <30 subsets were also performed.
Results
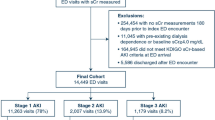
A total of 6877 ICU patients (4351 contrast, 2526 noncontrast) were included in the study. Following propensity score adjustment, the rates of AKI (31 vs. 34%, OR .88 (95% CI .75–1.05), p = .15), dialysis (2.0 vs. 1.7%, OR 1.20 (.66–2.17), p = .55), and mortality (12 vs. 14%, OR .87 (.69–1.10), p = .23) were not significantly higher in the contrast versus noncontrast group in the matched eGFR > 45 subset. Significantly higher rates of dialysis (6.7 vs. 2.5%, OR 2.72 (1.14–6.46), p = .0240) were observed in the contrast versus noncontrast group in the matched eGFR ≤ 45 subset.
Conclusions
Intravenous contrast material administration was not associated with an increased risk of AKI, emergent dialysis, and short-term mortality in ICU patients with pre-CT eGFR > 45. An increased risk of dialysis was observed in patients with pre-CT eGFR ≤ 45.

Similar content being viewed by others


References
Katzberg RW, Lamba R (2009) Contrast-induced nephropathy after intravenous administration: fact or fiction? Radiol Clin North Am 47:789–800
McDonald JS, McDonald RJ, Comin J, Williamson EE, Katzberg RW, Murad MH, Kallmes DF (2013) Frequency of acute kidney injury following intravenous contrast medium administration: a systematic review and meta-analysis. Radiology 267:119–128
ACR manual on contrast media. Version 10.2 (2016). https://www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/Contrast-Manual/2016_Contrast_Media.pdf?la=en
Solomon RJ, Mehran R, Natarajan MK, Doucet S, Katholi RE, Staniloae CS, Sharma SK, Labinaz M, Gelormini JL, Barrett BJ (2009) Contrast-induced nephropathy and long-term adverse events: cause and effect? Clin J Am Soc Nephrol 4:1162–1169
Stacul F, van der Molen AJ, Reimer P, Webb JA, Thomsen HS, Morcos SK, Almen T, Aspelin P, Bellin MF, Clement O, Heinz-Peer G (2011) Contrast induced nephropathy: updated ESUR Contrast Media Safety Committee guidelines. Eur Radiol 21:2527–2541
Katzberg RW, Newhouse JH (2010) Intravenous contrast medium-induced nephrotoxicity: is the medical risk really as great as we have come to believe? Radiology 256:21–28
Newhouse JH, RoyChoudhury A (2013) Quantitating contrast medium-induced nephropathy: controlling the controls. Radiology 267:4–8
Rao QA, Newhouse JH (2006) Risk of nephropathy after intravenous administration of contrast material: a critical literature analysis. Radiology 239:392–397
McDonald JS, McDonald RJ, Carter RE, Katzberg RW, Kallmes DF, Williamson EE (2014) Risk of intravenous contrast material-mediated acute kidney injury: a propensity score-matched study stratified by baseline-estimated glomerular filtration rate. Radiology 271:65–73
McDonald JS, McDonald RJ, Lieske JC, Carter RE, Katzberg RW, Williamson EE, Kallmes DE (2015) Risk of acute kidney injury, dialysis, and mortality in patients with chronic kidney disease after intravenous contrast material exposure. Mayo Clin Proc 90:1046–1053
McDonald RJ, McDonald JS, Bida JP, Carter RE, Fleming CJ, Misra S, Williamson EE, Kallmes DF (2013) Intravenous contrast material-induced nephropathy: causal or coincident phenomenon? Radiology 267:106–118
McDonald RJ, McDonald JS, Carter RE, Hartman RP, Katzberg RW, Kallmes DF, Williamson EE (2014) Intravenous contrast material exposure is not an independent risk factor for dialysis or mortality. Radiology 273:714–725
Cely CM, Schein RM, Quartin AA (2012) Risk of contrast induced nephropathy in the critically ill: a prospective, case matched study. Crit Care 16:R67
Ehrmann S, Badin J, Savath L, Pajot O, Garot D, Pham T, Capdevila X, Perrotin D, Lakhal K (2013) Acute kidney injury in the critically ill: is iodinated contrast medium really harmful? Crit Care Med 41:1017–1026
Wu MJ, Shu KH, Liu PH, Chiang PH, Cheng CH, Chen CH, Yu DM, Chuang YW (2010) High risk of renal failure in stage 3B chronic kidney disease is under-recognized in standard medical screening. J Chin Med Assoc 73:515–522
Herasevich V, Pickering BW, Dong Y, Peters SG, Gajic O (2010) Informatics infrastructure for syndrome surveillance, decision support, reporting, and modeling of critical illness. Mayo Clin Proc 85:247–254
Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A (2007) Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care 11:R31
R Development Core Team (2012) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna
Ho DE, Imai K, King G, Stuart EA (2011) MatchIt: nonparametric preprocessing for parametric causal inference. J Stat Softw 42(8). http://imai.princeton.edu/research/files/matchit.pdf
National Kidney Foundation (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39:(2 Suppl 1):1–266
Ng CS, Shaw AD, Bell CS, Samuels JA (2010) Effect of IV contrast medium on renal function in oncologic patients undergoing CT in ICU. AJR Am J Roentgenol 195:414–422
Chertow GM, Normand SL, McNeil BJ (2004) “Renalism”: inappropriately low rates of coronary angiography in elderly individuals with renal insufficiency. J Am Soc Nephrol 15(9):2462–2468
Acknowledgements
The authors thank Rickey Carter Ph.D. for his statistical expertise.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
JSM, DFK, and EEW report investigator-initiated research grants from GE Healthcare for CIN studies independent of the current study. DFK is a member of GE’s Cost Effectiveness Board independent of the current study. RJM and KK have no conflicts of interest to disclose.
Additional information
Take-home message: Recent controlled studies suggest that the incidence and severity of contrast-induced nephropathy, the development of acute kidney injury following administration of iodinated contrast material, have been overestimated. This study found that intravenous iodinated contrast material did not increase the risk of AKI in ICU patients with normal to mildly reduced renal function.
An erratum to this article is available at http://dx.doi.org/10.1007/s00134-017-4761-9.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
McDonald, J.S., McDonald, R.J., Williamson, E.E. et al. Post-contrast acute kidney injury in intensive care unit patients: a propensity score-adjusted study. Intensive Care Med 43, 774–784 (2017). https://doi.org/10.1007/s00134-017-4699-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-017-4699-y