
Abstract
Purpose
To study the effects of pretreatment with levosimendan (LEVO, a Ca2+-sensitizer and K +ATP channel opener) and/or the K +ATP channel antagonist glibenclamide (GLIB) on systemic hemodynamics, metabolism, and regional gastromucosal oxygenation during hypoxic hypoxemia.
Methods
Chronically instrumented, healthy dogs (24–32 kg, n = 6 per group, randomized cross-over design) were repeatedly sedated, mechanically ventilated (FiO2 ~0.3) and subjected to the following interventions: no pretreatment, LEVO pretreatment, GLIB pretreatment, or combined LEVO + GLIB pretreatment, each followed by hypoxic hypoxemia (FiO2 ~0.1). We measured cardiac output (CO, ultrasonic flow probes), oxygen consumption (VO2, indirect calorimetry), and gastromucosal microvascular hemoglobin oxygenation (μHbO2, spectrophotometry). Statistics: data are presented as mean ± SEM and compared by one-way ANOVA (direct drug effects within group) and two-way ANOVA (between all hypoxic conditions) both with Bonferroni corrections; p < 0.05.
Results
In LEVO-pretreated hypoxemia, CO was significantly higher compared to unpretreated hypoxemia. The increased CO was neither associated with an increased VO2 nor with markers of aggravated anaerobiosis (pH, BE, lactate). In addition, LEVO pretreatment did not further compromise gastromucosal μHbO2 in hypoxemia. After combined LEVO + GLIB pretreatment, systemic effects of GLIB were apparent, however, CO was significantly higher than during unpretreated and GLIB-pretreated hypoxemia, but equal to LEVO-pretreated hypoxemia, indicating that GLIB did not prevent the increased CO in LEVO-pretreated hypoxia.
Conclusions
LEVO pretreatment resulted in improved systemic circulation (CO) during hypoxemia without fueling systemic VO2, without aggravating systemic anaerobiosis markers, and without further compromising microvascular gastromucosal oxygenation. Thus, LEVO pretreatment may be an option to support the systemic circulation during hypoxia.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hypoxemia complicates critical care settings, ranging from progressed lung disease to certain medical interventions [1–3]. Clearly, reversing hypoxemia is pivotal [4], but adapting pharmacological interventions to support the subject during impending or actual hypoxemia also appears beneficial. Systemic hypoxemia triggers multiple patho-mechanisms [5] also affecting the cardiovascular system: among others, at the cardiac level hypoxia depresses cardiac function by myofilament Ca2+-desensitization [6, 7], and at the vascular level hypoxia triggers activation of K +ATP channels [8], facilitating blood flow to tissues otherwise at risk for hypoperfusion by intense vasoconstriction.
In this context, the inodilator levosimendan (LEVO) appears to be an attractive option to support the cardiovascular system at risk in (impending) hypoxemia since it acts both as cardiac myofilament Ca2+-sensitizer and K +ATP channel opener, thus reversing hypoxia-induced cardiodepression and supporting regional vasodilation. This appears to be particularly of interest in hypoxic settings, since LEVO putatively increases cardiac output (CO) partly independent of an additional increase in oxygen consumption (VO2) [9].
Hypoxia, like other cardiovascular stressors, triggers impairment of splanchnic oxygenation, likely through a combination of abnormal mesenteric perfusion [10–12] and hypoxemia. However, particularly the gastrointestinal mucosa is susceptible to hypoxia, and mucosal hypoxia appears to trigger the development of critical illness [13]. Thus, interventions intended to improve systemic (hemodynamic) variables during hypoxia should not further compromise regional mucosal circulation or oxygenation [14]. Therefore, in addition to systemic variables, we measured the effects on regional gastromucosal oxygenation.
Clinically, LEVO is primarily indicated for the treatment of acute and chronic ischemic cardiac failure, with promising clinical data available [15, 16]. Moreover, LEVO is also increasingly advocated to treat nonischemic cardiac failure, including septic or toxic cardiodepression [17–23]. The beneficial effects of LEVO, in addition to positive inotropic effects, may be caused by vasodilation [24]. Mechanistically, vasodilation by LEVO is mediated by activation of K +ATP channels, which also appear involved in the vasodilation triggered by hypoxia [8, 25].
These K +ATP channels, activated by LEVO or hypoxia, are pharmacologically blocked by glibenclamide (GLIB) [26–30]. In this context, GLIB pretreatment has previously been published as a research tool to study the contribution of GLIB-sensitive K +ATP channels to the effects of LEVO and other cardiovascular challenges [26–30]. Thus, to elucidate the contribution of K +ATP channels in the present study, we tested if K +ATP channel blockade by GLIB pretreatment would alter the (circulatory) condition during hypoxia, both with and without a LEVO pretreatment.
GLIB, based on the same mechanism, i.e., antagonizing K +ATP channel-dependent vasodilation, is of growing interest in intensive care medicine [31]. In this context, GLIB is studied as nonadrenergic vasopressor in various shock-related vasodilatory states, caused by excessive K +ATP channel activation. Examples for this therapeutic concept are septic or hemorrhagic vasodilation [32, 33]. In this regard, GLIB increases systemic vascular resistance and thus arterial blood pressure [32].
In the present study, the combination of LEVO (to increase cardiac contractility) and GLIB (to increase systemic vascular resistance) could achieve the putatively beneficial combination of antagonizing both possible cardiodepressant and vasodilatory effects of systemic hypoxia.
Materials and methods
The data derive from repetitive experiments on healthy dogs (foxhounds, n = 6, 24–32 kg) treated in accordance with the National Institutes of Health guidelines for animal care and with approval of the District Governmental Animal Investigation Committee.
For the continuous measurement of cardiac output (CO), ultrasonic flow transducers (S-series, Transonic, Ithaca, NY, USA) were chronically implanted around the pulmonary artery [34]. Before the experiments, food was withheld for 12 h. The experiments were performed under sedation with sevoflurane (end-tidal concentration 3.0 vol%, corresponding to ~1.25 MAC in dogs [35]) and neuromuscular block (rocuronium 0.6 mg kg−1, followed by 1.0 mg kg−1 h−1). Mechanical ventilation (FiO2 0.3; tidal volume 12.5 mL kg−1 in dogs [36], respiratory rate ~20 min−1) was adjusted to maintain normocapnia as verified by continuous capnography (end-tidal CO2 35 torr) and arterial blood gas analysis. The dogs were covered with warming blankets to maintain body temperature (~37.5°C, rectal thermoprobe).
Measurements
Systemic oxygen consumption
Systemic oxygen consumption (VO2) was measured continuously by indirect calorimetry (Deltatrac-II metabolic monitor, Datex, Helsinki, Finland) and thus was methodologically independent from the determination of CO and DO2 [9].
Systemic hemodynamics and oxygenation
We continuously measured heart rate (HR, electrocardiogram), mean arterial (aortic) pressure (MAP; P23ID, Elk Grove, CA, USA), central venous pressure (P23ID; right atrial catheter tip position confirmed by fluoroscopy), and ultrasound-derived CO (flowmeter T106, Transonic). At the end of each intervention, we performed transpulmonary thermodilution (PiCCO monitor with thermistor-tipped carotid catheter PV-2014L, Pulsion, Munich, Germany; measurements performed according to the manufacturer; with ~0.4 mL kg−1 iced saline) to determine the following: global end diastolic volume (GEDV), derived intrathoracic blood volume (ITBV), and extravascular lung water (EVLW). The PiCCO system also provided the pulse-contour-derived stroke volume variation (SVV) and the estimate of cardiac contractility +dP/dt max. This system is validated to measure EVLW in dogs [37] and has also been applied in other canine studies [38].
Intermittently we measured arterial blood gas tensions (PaO2, PaCO2) and acid/base-related variables [pH, base excess (BE); ABL-700, Radiometer, Copenhagen, Denmark; no buffer solutions were used]. Additionally, we determined arterial serum metabolites (glucose, lactate) and electrolytes ([K+], [Ca2+], [Na+], [Cl−]). According to standard formulas, we calculated systemic vascular resistance (SVR), arterial oxygen content (CaO2), and systemic oxygen transport (DO2).
Gastromucosal oxygenation
Gastromucosal oxygenation was continuously assessed by reflectance spectrophotometry [9, 39]. Briefly, light (502–628 nm) is transmitted to the tissue via a micro light guide, and the reflected light is analyzed for the percentage of oxygenated microvascular hemoglobin (μHbO2). The flexible probe (diameter 2.0 mm) was introduced into the stomach via an orogastric silicone tube (14 Charrière). During the experiments, correct probe position was confirmed by online evaluation of the signal quality (software version 2.0).
Experimental program
After induction (propofol 4 mg kg−1 i.v.) and endotracheal intubation, all catheters were inserted and 30 min was allowed to establish steady-state conditions. Blood was sampled for baseline analysis, and thereafter a randomization was performed to allocate the dogs to the experimental groups.
Hypoxia episodes
The hypoxic episodes were induced by switching FiO2 from 0.30 to 0.11 [40], as continuously measured (Capnomac ultima, Datex Instrumentarium, Helsinki, Finland). Each hypoxic episode was maintained for 15 min to allow steady states of the measured variables to be achieved.
Drugs
The agents LEVO and GLIB were infused as follows by a pressure-limited infusion pump via the central venous catheter.
LEVO
After baseline measurements, LEVO (Simdax, Abbott, Wiesbaden, Germany) was administered with an initial loading dose of 20.0 μg kg−1 over 15 min, followed by continuous infusion of 0.25 μg kg−1 min−1 for the remaining experimental period, a dosing regimen adapted from a similar canine model [9].
GLIB
GLIB (G0639, Sigma, Frankfurt, Germany), as K +ATP channel antagonist, was infused at a dose of 0.2 mg kg−1 over 10 min, and 30 min were allowed for stabilization. This dose was derived from previous canine studies addressing the contribution of K +ATP channels to the effects of LEVO and other cardiovascular modulators [26–30].
Experimental protocols
Group I
This protocol served to study the effects of hypoxia per se and to study the associated effects of GLIB pretreatment. After steady-state baseline measurements, a first hypoxic challenge was performed. After 60 min recovery from this hypoxia (measurements after 30 and 60 min recovery), GLIB was infused. Following this GLIB pretreatment, a second hypoxic episode was induced.
Group II
This protocol served to study the effects of LEVO pretreatment on hypoxia and further to study the role of GLIB pretreatment in this regard. After a baseline period, LEVO pretreatment was administered, and thereafter a first hypoxic episode was induced. After 60 min recovery from this hypoxia (measurements after 30 and 60 min recovery), with LEVO continuously infused, GLIB pretreatment was administered. Thereafter, with the combined LEVO + GLIB pretreatment, a second hypoxic challenge was induced.
Statistical analysis
Statistical analysis was performed using Prism software (version 5.0, GraphPad, La Jolla, CA, USA). Data are presented as absolute values of mean ± SEM for n = 6 animals per group in the manuscript and tables. Direct drug effects (before onset of hypoxemia) were described by one-way ANOVA for repeated measurements, corrected for multiple comparisons (Bonferroni). Differences during hypoxemia were tested both between groups (i.e., I and II) and between the hypoxia conditions (i.e., without and with GLIB pretreatment) using a two-way ANOVA, corrected for multiple comparisons (Bonferroni). Significance was assumed at p < 0.05.
Results
Hypoxia model
Hypoxia was induced by reducing FiO2 from 0.3 to 0.11, with maintenance of end-tidal CO2 (35 torr) and end-tidal sevoflurane (3.0 vol%) concentrations. This was achieved for all four hypoxic conditions without significant inter- or intragroup differences (Table 1).
Hypoxia in unpretreated animals
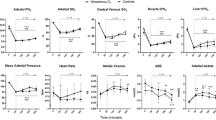
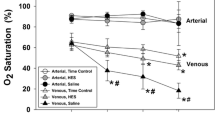
In our hypoxia model, reduction of FiO2 from 0.3 to 0.11 in unpretreated animals decreased PaO2 from 133 ± 9 to 39 ± 1 Torr and thereby SaO2 from 98 ± 0 to 68 ± 1%. Together with an unchanged Hb (stable at ~12.5 g dL−1, data not shown) this decreased CaO2 from 17.3 ± 0.8 to 11.7 ± 0.6 mL dL−1 (Table 1). At the regional level, gastromucosal μHbO2 decreased from 56 ± 3 to 32 ± 4% (Fig. 1). DO2 decreased from 14 ± 1 to 9 ± 1 mL kg−1 min−1, since CaO2 decreased without compensatory increase in CO. However, systemic VO2 was preserved at ~3.5 mL kg−1 min−1 (Table 2). Mechanical ventilation adjusted to maintain etCO2 at 35 Torr maintained PaCO2 at 35–38 Torr. Acid/base-related variables remained stable, i.e., pH at 7.35–7.37 and HCO3 − at ~20 mmol L−1. Glucose and lactate (Table 1) and all measured electrolytes remained close to baseline (data not shown).

Gastric mucosal microcirculatory hemoglobin oxygenation (μHbO2). Gastromucosal μHbO2 during normoxia (FiO2 ~0.3, thin outlined bars) and the two hypoxia episodes (FiO2 ~ 0.1, bold outlined bars) of the two experimental groups I (left bar per condition) and II (right bar per condition). Levosimendan was not given in group I, thus condition LEVO in group I is not determined (n.d.). Filling patterns: gray no pretreatment, downward stripes levosimendan (LEVO) pretreatment, upward stripes glibenclamide (GLIB) pretreatment, hatches levosimendan + glibenclamide pretreatment. Recovery-30 and recovery-60 are measurement points at 30 and 60 min of normoxic recovery. Mean ± SEM for n = 6 per group. aNo difference between hypoxia episodes, bsignificant difference within one group’s hypoxia episodes, csignificant difference between the two groups’ hypoxia episodes, * significant drug effects of LEVO and $ GLIB
Hypoxia in GLIB-pretreated animals
GLIB pretreatment, used to block GLIB-sensitive K +ATP channels, significantly increased SVR and significantly affected some blood-derived variables, e.g., it decreased arterial glucose concentration (Tables 1, 2).
Hypoxia after GLIB pretreatment resulted in a similar decreased CaO2 (11.1 ± 0.5 mL dL−1), compared to unpretreated animals (11.7 ± 0.6 mL dL−1). Also, no statistical differences were observed in ventilation- and acid/base-derived parameters (PaCO2, pH, and BE) and the O2-related variables μHbO2, DO2, and VO2 between these two hypoxic conditions. However, in GLIB-pretreated hypoxia, arterial lactate was significantly lower (~1.2 mmol L−1) compared to unpretreated hypoxia (~2.6 mmol L−1). Systemic hemodynamics (i.e., MAP and CO) did not differ between these two hypoxic episodes. Arterial electrolytes did not differ, and arterial glucose was significantly lower in GLIB-pretreated hypoxia (~80 mg dL−1) compared to unpretreated hypoxia (~110 mg dL−1) (Table 1).
Hypoxia in LEVO-pretreated animals
LEVO pretreatment at the macrocirculatory level significantly increased SV, CO, +dP/dt max, and DO2 and decreased SVR, without significant changes in HR. At the microcirculatory level, LEVO pretreatment significantly increased μHbO2 at a stable systemic SaO2.
Hypoxia after LEVO pretreatment resulted in a similar decrease in CaO2 to 10.3 ± 0.5 mL dL−1, compared to unpretreated animals. In LEVO-pretreated hypoxia, CO was significantly higher compared to unpretreated hypoxia, i.e., ~100 versus ~80 mL kg−1 min−1 (Figs. 2, 3). This was not paralleled by systemic VO2, which was comparable to unpretreated animals at ~3.5 mL kg−1 min−1. Also gastromucosal μHbO2 equally decreased in both unpretreated and LEVO-pretreated animals to ~30% (Fig. 1). Systemic vascular resistance was significantly lower in LEVO-pretreated hypoxia, compared to unpretreated hypoxia.

Cardiac output. Cardiac output during normoxia (FiO2 ~0.3, thin outlined bars) and the two hypoxia episodes (FiO2 ~0.1, bold outlined bars) of the two experimental groups I (left bar per condition) and II (right bar per condition). Levosimendan was not given in group I, thus condition LEVO in group I is not determined (n.d.). Filling patterns: gray no pretreatment, downward stripes levosimendan (LEVO) pretreatment, upward stripes glibenclamide (GLIB) pretreatment, hatches levosimendan + glibenclamide pretreatment. Recovery-30 and recovery-60 are measurement points at 30 and 60 min of normoxic recovery. Mean ± SEM for n = 6 per group. aNo difference between hypoxia episodes, bsignificant difference within one group’s hypoxia episodes, csignificant difference between the two groups’ hypoxia episodes, *significant drug effects of LEVO and $GLIB

Pressure-curve-derived contractility, +dP/dt max. Resulting +dP/dt max during normoxia (FiO2 ~0.3, thin outlined bars) and the two hypoxia episodes (FiO2 ~0.1, bold outlined bars) of the two experimental groups I (left bar per condition) and II (right bar per condition). Levosimendan was not given in group I, thus condition LEVO in group I is not determined (n.d.). Filling patterns: gray no pretreatment, downward stripes levosimendan (LEVO) pretreatment, upward stripes glibenclamide (GLIB) pretreatment, hatches levosimendan + glibenclamide pretreatment. Recovery-30 and recovery-60 are measurement points at 30 and 60 min of normoxic recovery. Mean ± SEM for n = 6 per group. aNo difference between hypoxia episodes, bsignificant difference within one group’s hypoxia episodes, csignificant difference between the two groups’ hypoxia episodes, *significant drug effects of LEVO and $GLIB
Hypoxia in LEVO- plus GLIB-pretreated animals
Administration of GLIB during LEVO infusion induced significant effects, e.g., GLIB significantly decreased serum glucose from 103 ± 4 to 87 ± 3 mg dL−1 (Table 1).
Hypoxic ventilation under combined pretreatment with LEVO and GLIB resulted in a PaO2 of 32 Torr. During hypoxia with LEVO + GLIB pretreatment, CaO2 tended to be lower compared to unpretreated hypoxia (9.4 ± 0.9 vs. 11.7 ± 0.6 mL dL−1), however, without statistical significance. CO was significantly higher than during hypoxia in solely GLIB-pretreated animals and did not differ from solely LEVO-pretreated animals (Fig. 2). SVR was significantly lower in LEVO + GLIB-pretreated hypoxia compared to GLIB-pretreated hypoxia. Systemic VO2 was comparable to all other hypoxic conditions at ~3.5 mL kg−1 min−1. Glucose, as expected, significantly decreased with GLIB.
Thermodilution-derived variables
Transpulmonary thermodilution (PiCCO) revealed no significant differences in the estimated blood volumes ITBV (~20 mL kg−1) and GEDV (~16 mL kg−1) or estimated EWLV (~9 mL kg−1) between the four hypoxemia conditions (data not shown).
Discussion
For the present study we developed a model of moderate hypoxic hypoxemia, adapting reported canine hypoxia models [40, 41]. Repetitive experiments were performed in a randomized mode on healthy, chronically instrumented dogs with intervals of ≥2 weeks to exclude carryover effects and to minimize interindividual differences. Furthermore, the use of chronically instrumented animals avoided acute, surgical instrumentation and thus confounders such as endocrine stress responses to surgery. In addition, our model allowed us to study the animals during sedation with sevoflurane and rocuronium alone, i.e., without need for analgesics or other confounding drugs [42].
In this study, two subsequent episodes of hypoxia were induced per group. While the first hypoxic episode served to elucidate the effect of LEVO pretreatment, the second hypoxic episode served to elucidate the role of K +ATP channels (by subsequently adding GLIB pretreatment, reported to block GLIB-sensitive K +ATP channels [26–30]). Between the two hypoxic episodes, an extended normoxic period was interposed to allow complete recovery of measured variables. In addition, to exclude the possibility that the first hypoxic episode was affecting the second with respect to measured variables, pilot experiments were performed, comparing a first with a second hypoxic period without adding any medication (i.e., no GLIB) in between. These pilot experiments demonstrated no differences between the first and second hypoxic episode, with respect to the measured variables.
Gastromucosal μHbO2 was continuously measured by reflectance spectrophotometry [43], with the light guide nontraumatically introduced via an orogastric tube [9, 39]. Reflectance spectrophotometry allows determination of microcirculatory oxygen availability [44], and gastric endoluminal reflectance spectroscopy has been reported predominantly to measure capillary hemoglobin oxygenation of the mucosa [45].
Both hypoxia and the administered drugs may affect pulmonary endothelial permeability. Thus, we assessed EVLW by the PiCCO system, a method validated in anaesthetized dogs [37]. The EVLW data do not support pulmonary edema as cause of the small but significant differences in PaO2 between distinct hypoxia conditions (i.e., slightly lower with LEVO and/or GLIB), rendering an altered pulmonary shunt, as also reported for other vasoactive agents [46], as the most likely explanation.
LEVO appears to be a promising candidate agent to support the cardiocirculatory system during hypoxemia, particularly because circulatory stimulation by LEVO is reportedly independent of metabolic stimulation [9]. Our data support this concept, demonstrating that LEVO pretreatment resulted in improved systemic circulation (CO) also during hypoxemia without fueling aerobic (VO2) metabolism. Thus, the pattern of increased CO at stable VO2 was present also during hypoxemia in LEVO-pretreated subjects and, in turn, other factors triggered by hypoxemia, e.g., changed pharmacology [47], did not alter this pattern. Measured key modulators of vascular tone (PaCO2, pH, temperature, arterial [K+] and [Ca2+]) did not differ between the hypoxemic episodes, supporting that LEVO-specific mechanisms cause the differences in cardiovascular response.
The present study was designed to suggest a concept to improve the condition of the subject before an anticipated hypoxemia evolves; however, the majority of clinical hypoxemia episodes occur unexpectedly. Therefore, future studies will have to demonstrate if our findings are confirmed in the clinically more likely setting, i.e., with LEVO administered in a therapeutic rather than prophylactic approach [24, 48].
Increased CO during hypoxemia after LEVO pretreatment, compared to unpretreated hypoxemia, was associated with an increased +dP/dt max, compatible with positive inotropic effects of LEVO by myocardial Ca2+ sensitizing. LEVO, besides acting as a cardiac Ca2+ sensitizer, also activates K +ATP channels. Physiologically, various K +ATP channel isoforms exist, classified by their respective sulfonylurea receptors (SUR) in pancreatic β-cells (SUR-1), and striated (SUR-2A) and smooth muscle cells (SUR-2B). Vascular smooth muscle K +ATP channels link regional metabolism to perfusion, since intracellular ATP depletion (e.g., during hypoxia) triggers these channels, leading to hyperpolarization and thus vasorelaxation [8]. However, excessive activation of these K +ATP channels is involved in multiple pathological vasodilatory states, e.g., septic shock [8, 25]. Thus, whether pharmacological activation of K +ATP channels under pathological conditions by LEVO is beneficial might also depend on the individual vasodilatory state. Pharmacologically, K +ATP channels are antagonized by sulfonylurea derivatives, with GLIB (glyburide) reported to unspecifically block all receptor isoforms, SUR-1, SUR-2A, and SUR-2B. GLIB has been reported to be effective as a K +ATP channel antagonist in dogs before, in similar dosages as applied in the present study [26–30]. Activity of GLIB in our model is suggested by the hypoglycemic response after GLIB pretreatment (SUR-1 effect), with arterial glucose decreased from baseline values of ~100 to ~50 mg dL−1 (end of experiments). In addition, GLIB pretreatment significantly increased SVR, suggesting (partial) blockade of vascular K +ATP channels.
Thus, although GLIB pretreatment significantly increased SVR in this model, the demonstrated marked hypoglycemic effect of GLIB may limit its clinical use.
Combined GLIB + LEVO pretreatment resulted in significantly higher CO and +dP/dt max than GLIB pretreatment alone during hypoxemia, compatible with the notion that mechanisms other than K +ATP channel opening contribute to LEVO effects, also during hypoxemia. Besides Ca2+ (re-)sensitization, LEVO’s action as a phosphodiesterase (PDE) inhibitor could also contribute. In this regard, other PDE-III inhibitors have demonstrated positive systemic and regional gastrointestinal mucosal effects during hypoxemia [14].
Despite significant systemic differences, regional gastromucosal oxygenation did not differ between LEVO-pretreated and unpretreated hypoxemia, which decreased equally to ~30%. Regional regulation of mucosal perfusion during hypoxemia could overrule the effects of LEVO, despite an increased CO and reduced SVR in LEVO-pretreated hypoxia. A possible mechanism is that local hypoxia activates vasodilatory K +ATP channels to such extents that LEVO can not confer significant additional vasodilation. Indeed after GLIB pretreatment, administered to block these vasodilatory K +ATP channels and thus to induce vasoconstriction, we observed clear trends towards lower μHbO2 both in LEVO-pretreated (from 32 ± 4 to 24 ± 4%) and unpretreated hypoxemia (from 30 ± 4 to 25 ± 3%). Interestingly, also in both groups arterial lactate concentrations were significantly lower after GLIB pretreatment. Since arterial pH and the other acid/base-related variables remained close to baseline under all hypoxemia conditions, we doubt that these significant differences in lactate concentration are caused by different perfusion states, rendering direct metabolic effects of GLIB more likely to contribute.
LEVO is clinically indicated for the treatment of chronic or acute cardiac failure, with promising results [15, 16], and indications have already extended to septic and toxic cardiac depression [17–23]. If our experimental data apply to the clinical setting, LEVO pretreatment may also be an option to support the cardiovascular system during hypoxemia, without fueling VO2, without aggravating systemic anaerobiosis markers, and without further compromising the regional gastromucosal oxygenation. Further studies will have to extend these experimental results to other hypoxia models and ultimately to the clinical setting.
References
Hilbert G, Gruson D, Vargas F, Valentino R, Favier JC, Portel L, Gbikpi-Benissan G, Cardinaud JP (2001) Bronchoscopy with bronchoalveolar lavage via the laryngeal mask airway in high-risk hypoxemic immunosuppressed patients. Crit Care Med 29:249–255
Jaber S, Amraoui J, Lefrant JY, Arich C, Cohendy R, Landreau L, Calvet Y, Capdevila X, Mahamat A, Eledjam JJ (2006) Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit. Crit Care Med 34:2355–2361
Mort TC (2005) Preoxygenation in critically ill patients requiring emergency tracheal intubation. Crit Care Med 33:2672–2675
Sud S, Friedrich JO, Taccone P, Polli F, Adhikari NK, Latini R, Pesenti A, Guérin C, Mancebo J, Curley MA, Fernandez R, Chan MC, Beuret P, Voggenreiter G, Sud M, Tognoni G, Gattinoni L (2010) Prone ventilation reduces mortality in patients with acute respiratory failure and severe hypoxemia. Intensive Care Med 36:585–599
Zaobornyj T, Gonzales GF, Valdez LB (2007) Mitochondrial contribution to the molecular mechanism of heart acclimatization to chronic hypoxia. Front Biosci 12:1247–1259
Allen DG, Orchard CH (1987) Myocardial contractile function during ischemia and hypoxia. Circ Res 60:153–168
Day SM, Westfall MV, Fomicheva EV, Hoyer K, Yasuda S, La Cross NC, D’Alecy LG, Ingwall JS, Metzger JM (2006) Histidine button engineered into cardiac troponin I protects the ischemic and failing heart. Nat Med 12:181–189
Landry DW, Oliver JA (2001) The pathogenesis of vasodilatory shock. N Engl J Med 345:588–595
Schwarte LA, Picker O, Bornstein SR, Fournell A, Scheeren TW (2005) Levosimendan is superior to milrinone and dobutamine in selectively increasing microvascular gastric mucosal oxygenation in dogs. Crit Care Med 33:135–142
Mathie RT, Blumgart LH (1983) Effect of denervation on the hepatic haemodynamic response to hypercapnia and hypoxia in the dog. Pflugers Arch 397:152–157
Marshall JM, Metcalfe JD (1989) Analysis of factors that contribute to cardiovascular changes induced in the cat by graded levels of systemic hypoxia. J Physiol 412:429–448
Leach RM, Robertson TP, Twort CH, Ward JP (1994) Hypoxic vasoconstriction in rat pulmonary and mesenteric arteries. Am J Physiol 266:223–231
Sandek A, Rauchhaus M, Anker SD, von Haehling S (2008) The emerging role of the gut in chronic heart failure. Curr Opin Clin Nutr Metab Care 11:632–639
Satoh T, Morisaki H, Ai K, Kosugi S, Yamamoto M, Serita R, Kotake Y, Takeda J (2003) Olprinone, a phosphodiesterase III inhibitor, reduces gut mucosal injury and portal endotoxin level during acute hypoxia in rabbits. Anesthesiology 98:1407–1414
Delaney A, Bradford C, McCaffrey J, Bagshaw SM, Lee R (2010) Levosimendan for the treatment of acute severe heart failure: a meta-analysis of randomised controlled trials. Int J Cardiol 138:281–289
Landoni G, Mizzi A, Biondi-Zoccai G, Bignami E, Prati P, Ajello V, Marino G, Guarracino F, Zangrillo A (2010) Levosimendan reduces mortality in critically ill patients. A meta-analysis of randomized controlled studies. Minerva Anestesiol 76:276–286
Parissis JT, Rafouli-Stergiou P, Stasinos V, Psarogiannakopoulos P, Mebazaa A (2010) Inotropes in cardiac patients: update 2011. Curr Opin Crit Care 16:432–441
Leppikangas H, Ruokonen E, Rutanen J, Kiviniemi V, Lindgren L, Kurola J (2009) Levosimendan as a rescue drug in experimental propranolol-induced myocardial depression: a randomized study. Ann Emerg Med 54:811–817
Creteur J, Bouckaert Y, Melot C, Vincent JL (2006) Effects of levosimendan on systemic and regional hemodynamics in septic myocardial depression. Intensive Care Med 32:790
DeBacker D, Taccone FS, Radermacher P (2007) Levosimendan in septic shock: another piece in the puzzle, but many pieces are still lacking. Intensive Care Med 33:403–405
Dubin A, Murias G, Sottile JP, Pozo MO, Barán M, Edul VS, Canales HS, Etcheverry G, Maskin B, Estenssoro E (2007) Effects of levosimendan and dobutamine in experimental acute endotoxemia: a preliminary controlled study. Intensive Care Med 33:485–494
Morelli A, De Castro S, Teboul JL, Singer M, Rocco M, Conti G, De Luca L, Di Angelantonio E, Orecchioni A, Pandian NG, Pietropaoli P (2005) Effects of levosimendan on systemic and regional hemodynamics in septic myocardial depression. Intensive Care Med 31:638–644
Scheiermann P, Ahluwalia D, Hoegl S, Dolfen A, Revermann M, Zwissler B, Muhl H, Boost KA, Hofstetter C (2009) Effects of intravenous and inhaled levosimendan in severe rodent sepsis. Intensive Care Med 35:1412–1419
Morelli A, Ertmer C, Pietropaoli P, Westphal M (2009) Reducing the risk of major elective non-cardiac surgery: is there a role for levosimendan in the preoperative optimization of cardiac function? Curr Drug Targets 10:863–871
Landry DW, Oliver JA (1992) The ATP-sensitive K+ channel mediates hypotension in endotoxemia and hypoxic lactic acidosis in dog. J Clin Invest 89:2071–2074
Fukunari A, Miyai H, Shinagawa K, Kawahara K, Nakajima T (1997) Y-26763 protects the canine heart from a stunning injury through opening of the KATP channels. Eur J Pharmacol 323:197–204
Ito M, Pride HP, Zipes DP (1994) Glibenclamide enhances but pinacidil reduces attenuation in sympathetic responsiveness after acute coronary artery occlusion. Circ Res 75:379–392
Kersten JR, Montgomery MW, Pagel PS, Warltier DC (2000) Levosimendan, a new positive inotropic drug, decreases myocardial infarct size via activation of K(ATP) channels. Anesth Analg 90:5–11
Yao Z, Gross GJ (1993) Glibenclamide antagonizes adenosine A1 receptor-mediated cardioprotection in stunned canine myocardium. Circulation 88:235–244
Yao Z, Gross GJ (1994) A comparison of adenosine-induced cardioprotection and ischemic preconditioning in dogs. Efficacy, time course, and role of KATP channels. Circulation 89:1229–1236
Lange M, Morelli A, Westphal M (2008) Inhibition of potassium channels in critical illness. Curr Opin Anaesthesiol 21:105–110
Maybauer DM, Salsbury JR, Westphal M, Maybauer MO, Salzman AL, Szabó C, Westphal-Varghese BB, Traber LD, Traber DL (2004) The ATP-sensitive potassium-channel inhibitor glibenclamide improves outcome in an ovine model of hemorrhagic shock. Shock 22:387–391
Musser JB, Bentley TB, Griffith S, Sharma P, Karaian JE, Mongan PD (2004) Hemorrhagic shock in swine: nitric oxide and potassium sensitive adenosine triphosphate channel activation. Anesthesiology 101:399–408
Schwarte LA, Picker O, Bornstein SR, Fournell A, Scheeren TW (2005) Levosimendan is superior to milrinone and dobutamine in selectively increasing microvascular gastric mucosal oxygenation in dogs. Crit Care Med 33:135–142
Boller M, Moens Y, Kästner SB, Bettschart-Wolfensberger R (2005) Closed system anaesthesia in dogs using liquid sevoflurane injection; evaluation of the square-root-of-time model and the influence of CO2 absorbent. Vet Anaesth Analg 32:168–177
Blumenthal SR, Skoula CM, Gordon BE (1998) Relationship between inspiratory pressure and tidal volume in the anesthetized canine. Lab Anim Sci 48:69–73
Katzenelson R, Perel A, Berkenstadt H, Preisman S, Kogan S, Sternik L, Segal E (2004) Accuracy of transpulmonary thermodilution versus gravimetric measurement of extravascular lung water. Crit Care Med 32:1550–1554
Kim HK, Pinsky MR (2008) Effect of tidal volume, sampling duration, and cardiac contractility on pulse pressure and stroke volume variation during positive-pressure ventilation. Crit Care Med 36:2858–2862
Schwartges I, Schwarte LA, Fournell A, Scheeren TW, Picker O (2008) Hypercapnia induces a concentration-dependent increase in gastric mucosal oxygenation in dogs. Intensive Care Med 34:1898–1906
Kohzuki H, Sakata S, Misawa H, Takaki M (2002) O2 delivery and the venous PO2–O2 uptake relationship in pump-perfused canine muscle. Exp Physiol 87:53–61
Kato R, Sato J, Nishino T (1998) Milrinone decreases both pulmonary arterial and venous resistances in the hypoxic dog. Br J Anaesth 81:920–924
Ebert TJ, Ficke DJ, Arain SR, Holtz MN, Shankar H (2005) Vasodilation from sufentanil in humans. Anesth Analg 101:1677–1680
Knotzer H, Maier S, Dünser MW, Hasibeder WR, Hausdorfer H, Brandner J, Torgersen C, Ulmer H, Friesenecker B, Iannetti C, Pajk W (2006) Arginine vasopressin does not alter mucosal tissue oxygen tension and oxygen supply in an acute endotoxemic pig model. Intensive Care Med 32:170–174
Jakob SM, Takala J (2002) ARDS. Monitoring tissue perfusion. Crit Care Clin 18:143–163
Severinghaus JW (2003) Continuous positive airway pressure, shock therapy, and gastric mucosal oxygenation. Crit Care Med 31:1870–1871
Adnot S, Radermacher P, Andrivet P, Dubois-Rande JL, Dupeyrat A, Lemaire F (1991) Effects of sodium-nitroprusside and urapidil on gas exchange and ventilation-perfusion relationships in patients with congestive heart failure. Eur Respir J 4:69–75
Mace SE (1990) Effect of hypoxemia on pharmacokinetics of endotracheal lidocaine in dogs. Resuscitation 20:41–48
Brezina A, Riha H, Pirk J (2009) Prophylactic application of levosimendan in cardiac surgical patients with severe left ventricle dysfunction. Exp Clin Cardiol 14:31–34
Conflict of interest
None of the authors is affiliated with any company involved. Funding came from departmental sources.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is discussed in the editorial available at doi:10.1007/s00134-011-2204-6.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Schwarte, L.A., Schwartges, I., Thomas, K. et al. The effects of levosimendan and glibenclamide on circulatory and metabolic variables in a canine model of acute hypoxia. Intensive Care Med 37, 701–710 (2011). https://doi.org/10.1007/s00134-011-2144-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-011-2144-1