
Dear Editor,
Implementing lung protective ventilation while assuring acceptable arterial oxygenation and carbon dioxide removal in patients affected by severe acute respiratory failure and very low respiratory system compliance is a major challenge [1]. Extracorporeal membrane oxygenation (ECMO) may guarantee viable blood gases [2] and allow the use of assisted rather than controlled mechanical ventilation. This, in turn, will achieve improved respiratory muscle function, better gas exchange and decreased sedation level [3]. Pressure support ventilation (PSV), however, may be difficult to implement in patients with very low compliance [3]. In these patients, peak inspiratory flow is reached rapidly and the expiratory phase of the ventilator may start while the patient is still inspiring. This mechanism may lead to patient discomfort, asynchrony and possibly desaturation and barotrauma. We reasoned that neurally adjusted ventilatory assist (NAVA) may overcome this limitation as expiratory cycling time is based on diaphragmatic electrical activity (EAdi) and should adapt better to the patient’s own respiratory pattern [4].
A 58-year-old male patient (predicted body weight 90 kg) developed acute respiratory failure from exacerbation of idiopathic pulmonary fibrosis [5]. He was severely hypoxaemic and hypercapnic. Therefore ECMO was initiated while the patient was undergoing noninvasive ventilation. After 7 days, his respiratory function further declined and he was intubated and mechanically ventilated. On ECMO day 14, the patient was on controlled ventilation with tidal volume (V T) 2 ml/kg, respiratory rate (RR) 15 bpm, positive end expiratory pressure (PEEP) 10 cmH2O and inspired oxygen fraction (FiO2) 100%. ECMO blood flow was 2.3 l/min with 5 l/min of pure oxygen sweep gas flow. Arterial haemoglobin saturation (SatO2) was 75% and compliance was 7 ml/cmH2O. We tested each of the assisted ventilatory strategy listed below for 30 min, leaving PEEP, FiO2 and ECMO settings unchanged, with the following observations:
-
1.
PSV30 (PSV 12 cmH2O above PEEP, expiration cycling time 30% of flow peak value): V T was 2 ml/kg and RR 22 bpm; patient inspiration overlapped machine expiration and this constantly triggered a second breath (“double hit breaths”) (Fig. 1, PSV30); global asynchrony index (AI) [6] was ≥10%; patient respiratory drive was high (p0.1 = 3.3 cmH2O, peak EAdi = 12 μV); SatO2 decreased to 73%.
Fig. 1 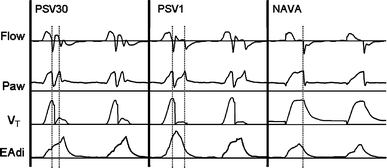
Airway flow (Flow), airway pressure (Paw), tidal volume (V T) and diaphragm electrical activity (EAdi) of a patient with extremely low compliance of the respiratory system during pressure support ventilation with expiration cycling set at 30% of peak inspiratory flow (PSV30), pressure support ventilation with expiration cycling set at 1% of peak inspiratory flow (PSV1) and neurally adjusted ventilatory assist with gain 2 cmH2O/μV (NAVA). The dashed lines represent the starting of the expiratory phase of the ventilator
-
2.
PSV1 (PSV 12 cmH2O and cycling at 1%): V T was 1.9 ml/kg and RR 22 bpm; reduction of the cycling-off criterion (until the latest allowed by the ventilator) did not improve synchrony and the inspiratory phase of the ventilator was still shorter than the patient’s own, yielding double-hit breaths (Fig. 1, PSV1); AI remained ≥10%, p0.1 increased to 3.7 cmH2O and peak EAdi to 13 μV; SatO2 remained stable at 73%.
-
3.
NAVA (gain 2 cmH2O/μV, to achieve the same peak airway pressure as in PSV; limit of airway pressure set on ventilator 35 cmH2O): V T ranged between 1.9 and 2.1 ml/kg and RR was 23 bpm; airway pressure increased following the shape of the patient’s EAdi, then reached a plateau and inspiratory flow zeroed, until EAdi had decreased to 70% of its peak value (i.e. NAVA cycling-off criterion, Fig. 1). AI lowered to <10%, respiratory drive decreased (p0.1 = 0.3 cmH2O, peak EAdi = 5.9 μV) and SatO2 increased to 77%. Interestingly, airway pressure waveforms in our patient (Fig. 1, NAVA) differed from those found in previous studies on NAVA [7] where pressure increased and decreased without reaching a plateau. Usually, a plateau during NAVA is seen when the airway pressure limit is reached, but this was not the case in our patient as the limit was 2–8 cmH2O higher than the actual plateau pressures. Airway pressure in our patient instead reached a plateau probably because of his/her slow rate of decrease in EAdi from the peak value. In the presence of early flow termination due to low compliance, the slow rate of decrease in EAdi yielded a longer time between peak pressure and cycling-off, during which airway flow was null and airway pressure was held at a plateau.

By maintaining the above-mentioned NAVA settings, we managed the patient for several days without relevant asynchrony issues.
In conclusion, we report here the successful application of NAVA to maintaining assisted ventilation in a patient with extremely low respiratory system compliance undergoing ECMO.
References
Terragni PP, Rosboch G, Tealdi A, Corno E, Menaldo E, Davini O, Gandini G, Herrmann P, Mascia L, Quintel M, Slutsky AS, Gattinoni L, Ranieri VM (2007) Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am J Respir Crit Care Med 175:160–166
Brogan TV, Thiagarajan RR, Rycus PT, Bartlett RH, Bratton SL (2009) Extracorporeal membrane oxygenation in adults with severe respiratory failure: a multi-center database. Intensive Care Med 35:2105–2114
Cereda M, Foti G, Marcora B, Gili M, Giacomini M, Sparacino ME, Pesenti A (2000) Pressure support ventilation in patients with acute lung injury. Crit Care Med 28:1269–1275
Brander L, Sinderby C, Lecomte F, Leong-Poi H, Bell D, Beck J, Tsoporis JN, Vaschetto R, Schultz MJ, Parker TG, Villar J, Zhang H, Slutsky AS (2009) Neurally adjusted ventilatory assist decreases ventilator-induced lung injury and non-pulmonary organ dysfunction in rabbits with acute lung injury. Intensive Care Med 35:1979–1989
Porte A, Stoeckel ME, Mantz JM, Tempe JD, Jaeger A, Batzenschlager A (1978) Acute interstitial pulmonary fibrosis. Comparative light and electron microscopic study of 19 cases. Pathogenic and therapeutic implications. Intensive Care Med 4:181–191
Vignaux L, Vargas F, Roeseler J, Tassaux D, Thille AW, Kossowsky MP, Brochard L, Jolliet P (2009) Patient-ventilator asynchrony during non-invasive ventilation for acute respiratory failure: a multicenter study. Intensive Care Med 35:840–846
Spahija J, de Marchie M, Albert M, Bellemare P, Delisle S, Beck J, Sinderby C (2010) Patient-ventilator interaction during pressure support ventilation and neurally adjusted ventilatory assist. Crit Care Med 38:518–526
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mauri, T., Bellani, G., Foti, G. et al. Successful use of neurally adjusted ventilatory assist in a patient with extremely low respiratory system compliance undergoing ECMO. Intensive Care Med 37, 166–167 (2011). https://doi.org/10.1007/s00134-010-2030-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-010-2030-2