
Abstract
Objective
To determine the incidence, risk factors, and prognostic implications of serum creatinine changes following major vascular surgery.
Design
Observational study.
Settings
University hospital.
Patients
Cohort of 599 consecutive patients undergoing elective abdominal aortic surgery.
Interventions
Review of prospectively collected data from 1993 to 2004.
Measurements and results
The receiver-operator characteristic (ROC) curve analysis was used to detect the best threshold for postoperative elevation in serum creatinine (Δ Creat) in relation to major complications. A cut-off value of +0.5 mg/dl was selected to define renal dysfunction (RD0.5 group, n = 91; no RD0.5, n = 508) that was associated with higher mortality (7.7% in RD0.5 group vs 1.4% in no RD0.5 group, P < 0.05), rate of admission to the ICU (34% vs 13%, P < 0.05), and incidence of cardiovascular (9% vs 4%, P < 0.05), respiratory (21% vs 7%, P < 0.05), surgical (24% vs 10%, P < 0.05), and septic complications (9% vs 3%, P < 0.05).
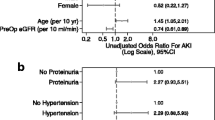
After multivariate analysis with logistic regression, renal dysfunction was independently related to low preoperative creatinine clearance [< 40 ml/min; odds ratio (OR) 1.5, 95% confidence interval (CI) 1.1–3.9], prolonged renal ischemic time (> 40 min; OR, 3.8, 95% CI, 1.9–7.2), blood transfusion (> 5 units; OR, 1.9, 95% CI 1.2–6.1), and rhabdomyolysis (OR, 3.6, 95% CI 1.7–7.9).
Conclusions
Postoperative RD0.5 (Δ Creat > 0.5 mg/dl) occurs in 15% of vascular patients and carries a bad prognosis. Preoperative renal insufficiency and factors related to the complexity of surgery are the main predictors of renal dysfunction.


Similar content being viewed by others


References
Sear JW (2005) Kidney dysfunction in the postoperative period. Br J Anaesth 95:20–32
Hertzer NR, Mascha EJ, Karafa MT, O'Hara PJ, Krajewski LP, Beven EG (2002) Open infrarenal abdominal aortic aneurysm repair: the Cleveland Clinic experience from 1989 to 1998. J Vasc Surg 35:1145–1154
Breckwoldt WL, Mackey WC, Belkin M, O'Donnell TF Jr (1992) The effect of suprarenal cross-clamping on abdominal aortic aneurysm repair. Arch Surg 127:520–524
Powell RJ, Roddy SP, Meier GH, Gusberg RJ, Conte MS, Sumpio BE (1997) Effect of renal insufficiency on outcome following infrarenal aortic surgery. Am J Surg 174:126–130
Fleron MH, Weiskopf RB, Bertrand M, Mouren S, Eyraud D, Godet G, Riou B, Kieffer E, Coriat P (2003) A comparison of intrathecal opioid and intravenous analgesia for the incidence of cardiovascular, respiratory, and renal complications after abdominal aortic surgery. Anesth Analg 97:2–12
Ryckwaert F, Alric P, Picot MC, Djoufelkit K, Colson P (2003) Incidence and circumstances of serum creatinine increase after abdominal aortic surgery. Intensive Care Med 29:1821–1824
Prinssen M, Verhoeven EL, Buth J, Cuypers PW, van Sambeek MR, Balm R, Buskens E, Grobbee DE, Blankensteijn JD (2004) A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med 351:1607–1618
Kudo FA, Nishibe T, Miyazaki K, Murashita T, Yasuda K, Ando M, Nishibe M (2004) Postoperative renal function after elective abdominal aortic aneurysm repair requiring suprarenal aortic cross-clamping. Surg Today 34:1010–1013
Braams R, Vossen V, Lisman BA, Eikelboom BC (1999) Outcome in patients requiring renal replacement therapy after surgery for ruptured and non-ruptured aneurysm of the abdominal aorta. Eur J Vasc Endovasc Surg 18:323–327
Sarac TP, Clair DG, Hertzer NR, Greenberg RK, Krajewski LP, O'Hara PJ, Ouriel K (2002) Contemporary results of juxtarenal aneurysm repair. J Vasc Surg 36:1104–1111
Aronson S, Blumenthal R (1998) Perioperative renal dysfunction and cardiovascular anesthesia: concerns and controversies J Cardiothorac Vasc Anesth 12:567–586
Lieberthal W, Nigam SK (2000) Acute renal failure. II Experimental models of acute renal failure: imperfect but indispensable. Am J Physiol Renal Physiol 278:F1–F12
Laukontaus SJ, Lepantalo M, Kantonen I, Pettila V (2005) Prediction of survival after 48-h of intensive care following open surgical repair of ruptured abdominal aortic aneurysm. Eur J Vasc Endovasc Surg 30:509–515
Zacharias M, Gilmore IC, Herbison GP, Sivalingam P, Walker RJ (2005) Interventions for protecting renal function in the perioperative period. Cochrane Database Syst Rev 3:CD003590
Tang IY, Murray PT (2004) Prevention of perioperative acute renal failure: what works? Best Pract Res Clin Anaesthesiol 18:91–111
Cockcroft DW, Gault MH (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16:31–41
Moreno R, Vincent JL, Matos R, Mendonca A, Cantraine F, Thijs L, Takala J, Sprung C, Antonelli M, Bruining H, Willats S (1999) The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Working Group on Sepsis related Problems of the ESICM. Intensive Care Med 25(7):686–696
Charlson ME, MacKenzie CR, Gold JP, Shires DT (1989) Postoperative changes in serum creatinine. When do they occur and how much is important? Ann Surg 209(3):328–333
Van Den Noortgate NJ, Janssens WH, Delanghe JR, Afschrift MB, Lameire NH (2002) Serum cystatin C concentration compared with other markers of glomerular filtration rate in the old. J Am Geriatr Soc 50:1278–1282
Daniel JP, Chantrel F, Offner M, Moulin B, Hannedouche T (2004) Comparison of cystatin C, creatinine and creatinine clearance vs. GFR for detection of renal failure in renal transplant patients. Ren Fail 26(3):253–257
Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W, Bauer P, Hiesmayr M (2004) Minimal changes of serum creatinine predict prognosis in patients after cardiothoracic surgery: a prospective cohort study. J Am Soc Nephrol 15:1597–1605
Coselli JS, LeMaire SA, Conklin LD, Koksoy C, Schmittling ZC (2002) Morbidity and mortality after extent II thoracoabdominal aortic aneurysm repair. Ann Thorac Surg 73:1107–1116
Huynh TT, Miller CC, 3rd, Estrera AL, Sheinbaum R, Allen SJ, Safi HJ (2002) Determinants of hospital length of stay after thoracoabdominal aortic aneurysm repair. J Vasc Surg 35:648–653
Ryckwaert F, Boccara G, Frappier JM, Colson PH (2002) Incidence, risk factors, and prognosis of a moderate increase in plasma creatinine early after cardiac surgery. Crit Care Med 30:1495–1498
Johnston KW (1989) Multicenter prospective study of nonruptured abdominal aortic aneurysm. Part II. Variables predicting morbidity and mortality. J Vasc Surg 9:437–447
Bown MJ, Nicholson ML, Bell PR, Sayers RD (2001) Cytokines and inflammatory pathways in the pathogenesis of multiple organ failure following abdominal aortic aneurysm repair. Eur J Vasc Endovasc Surg 22:485–527
Thakar CV, Worley S, Arrigain S, Yared JP, Paganini EP (2005) Influence of renal dysfunction on mortality after cardiac surgery: modifying effect of preoperative renal function. Kidney Int 67:1112–1119
O'Brien MM, Gonzales R, Shroyer AL, Grunwald GK, Daley J, Henderson WG, Khuri SF, Anderson RJ (2002) Modest serum creatinine elevation affects adverse outcome after general surgery. Kidney Int 62:585–592
Jean-Claude JM, Reilly LM, Stoney RJ, Messina LM (1999) Pararenal aortic aneurysms: the future of open aortic aneurysm repair. J Vasc Surg 29:902–912
Krause SM, Walsh TF, Greenlee WJ, Ranaei R, Williams DL, Jr., Kivlighn SD (1997) Renal protection by a dual ETA/ETB endothelin antagonist, L-754,142, after aortic cross-clamping in the dog. J Am Soc Nephrol 8:1061–1071
Wahlberg E, Dimuzio PJ, Stoney RJ (2002) Aortic clamping during elective operations for infrarenal disease: the influence of clamping time on renal function. J Vasc Surg 36:13–18
Bertrand M, Godet G, Fleron MH, Bernard MA, Orcel P, Riou B, Kieffer E, Coriat P (1997) Lumbar muscle rhabdomyolysis after abdominal aortic surgery. Anesth Analg 85:11–15
Holt SG, Moore KP (2001) Pathogenesis and treatment of renal dysfunction in rhabdomyolysis. Intensive Care Med 27:803–811
Concato J, Feinstein AR, Holford TR (1993) The risk of determining risk with multivariate models. Ann Intern Med 118:201–210
Williams JL, Hathaway CA, Kloster KL, Layne BH (1997) Low power, type II errors, and other statistical problems in recent cardiovascular research. Am J Physiol 273:H487–H493
Urbach DR, Baxter NN (2004) Does it matter what a hospital is “high volume” for? Specificity of hospital volume-outcome associations for surgical procedures: analysis of administrative data. Qual Saf Health Care 13(5):379–383
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Definitions of major non-fatal complications
Cardiovascular
-
1.
Myocardial infarct: typical rise and fall of CPK (> 120 U/l) and CK-MB/CPK ≥ 6% or troponin-I ≥ 1.5 ng/ml with at least one of the following criteria: ischemic symptoms, development of pathological Q waves on the ECG, ST segment elevation or depression (≥ 1 mm) or coronary artery intervention
-
2.
Arrhythmias: supraventricular and ventricular tachyarrhythmias on ECG requiring anti-arrhythmic medications and/ or an electrical cardioversion
-
3.
Congestive heart failure: need for sympathomimetic support, diuretics, or vasodilators consistent with clinical, hemodynamic (pulmonary artery pressure ≥ 15 mmHg), and radiological evidence of pulmonary congestion
Cerebral
Stroke: focal neurological deficit (transient or permanent)
Respiratory
-
1.
Atelectasis: lobar collapse (chest X-rays), need for CPAP and/or bronchoscopy
-
2.
Bronchopneumonia: temperature > 38°C, hyperleukocytosis (neutrophils), new lung infiltration (chest X-rays), positive culture (bronchial secretions or alveolar fluid)
-
3.
Prolonged mechanical ventilation ≥ 24 h
Surgical
-
1.
Re-operation for bleeding
-
2.
Re-operation for ischemia
Sepsis
Systemic inflammatory response syndrome (SIRS) associated with an infection (positive culture of blood, urine, bronchoalveolar lavage fluid or other internal fluid specimen):
-
Body temperature < 35.6° or > 38.3°C
-
Tachycardia (> 90 beats/min)
-
Ventilatory frequency > 20 bpm or PaCO2 < 4.3 kPa
-
White blood cells > 12 × 109/l or < 4 × 109/l, or 10% immature neutrophils
Rhabdomyolysis
Creatine phosphokinase (CPK) value > 1700 U/l, corresponding to the mean value +2 SD of maximum CPK value observed after peripheral vascular surgery in our institution, in the absence of myocardial infarct (see above).
Rights and permissions
About this article
Cite this article
Ellenberger, C., Schweizer, A., Diaper, J. et al. Incidence, risk factors and prognosis of changes in serum creatinine early after aortic abdominal surgery. Intensive Care Med 32, 1808–1816 (2006). https://doi.org/10.1007/s00134-006-0308-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-006-0308-1