
Abstract
Objective
To study the relation between the liver tissue oxygenation index (TOI), transcutaneously measured with spatially resolved spectroscopy (a new method of near-infrared spectroscopy or NIRS), the mixed venous oxygen saturation and the blood flow in the different parts of the splanchnic circulation in newborn piglets.
Design
Tissue oxygenation index of the liver was measured in six newborn piglets at 33°C, 35°C, 37°C and after a decrease in arterial carbon dioxide pressure (PaCO2).
Measurements
Mixed venous oxygen saturation, blood gas analysis and peripheral oxygen saturation were measured at each step. Gastric, proximal jejunal, midgut, distal ileal, splenic and hepatic arterial blood flow were measured by injection of coloured microspheres into the left atrium. NIRS optodes were attached to the skin over the liver and TOI was calculated.
Results
No significant changes of TOI of the liver were seen during the increase in temperature or change in PaCO2. TOI correlated well with mixed venous oxygen saturation (r=0.85), the mid-ileal blood flow (r=0.57) and the distal ileal blood flow (r=0.72).
Conclusions
Measurement of the TOI of the liver might be a non-invasive way to measure the distal ileal blood flow.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Spatially resolved spectroscopy (SRS) measures haemoglobin oxygen saturation in a non-invasive way [1, 2]. In contrast to differential near-infrared spectroscopy (NIRS), this technique yields an absolute value [tissue oxygenation index (TOI)]. Several reports have described the transcutaneous measurement of TOI of the liver by means of NIRO 300 [3, 4, 5]. When measuring the oxygenation of the liver, the blood in the total vascular network of the liver will be measured. This vascular network is supplied by three main vessels. The portal vein drains the venous blood of the splanchnic system. The hepatic artery and its branches join the branches of the portal vein at the level of the sinusoids and are distributed to the same territory in this way [6]. Seventy-five percent of the global hepatic blood supply is derived from the portal vein and 25% from the hepatic artery. Teller et al. [7] were the first to draw attention to a decrease in TOI of the liver during feeding in neonates, suggesting that this could reflect the splanchnic circulation.
To investigate the TOI of the liver, the following hypotheses were tested:
-
1.
The TOI of the liver correlates well with the mixed venous oxygen saturation.
-
2.
The TOI of the liver correlates well with the liver blood flow.
-
3.
There is a relation between the splanchnic flow and the tissue oxygenation of the liver.
The ethical committee for animal work of the KU Leuven approved the experiment.
Methods
Animal preparation
Newborn piglets (6–36 h of age) were studied. Premedication was given and intubation with a 3.5 mm ID uncuffed tube was performed. The piglet was fully anaesthetised and ventilated with an Engström ventilator. Ventilation was started with an extra dead space between the endotracheal tube and the ventilator circuit. Peripheral oxygen saturation, ECG and rectal temperature were measured at the start. Denudation of the right femoral artery was performed. The probe was placed cutaneously over the liver region after palpation of the liver. A NIRS patch was placed on the skin over the anterior liver surface and fixed with a running suture. Left thoracotomy was performed to insert a left atrial catheter and a catheter in the pulmonary artery.
Experimental protocol
The experiment was performed in four steps. Firstly, the piglet was further cooled to 33°C and in the second and third steps rewarmed to 35°C and 37°C. As a fourth step the extra dead space was removed to achieve a change in arterial carbon dioxide pressure (PaCO2) without change in minute ventilation. At each step blood samples (0.2 ml) were taken from the femoral and the pulmonary arteries, just before the coloured microspheres were injected. Each blood sample was analysed for PaCO2, arterial oxygen pressure (PaO2), pH, haemoglobin and the bicarbonate radical HCO3. At each step polystyrene microspheres of different colours (white, eosin, blue, violet and yellow) were injected into the left atrium. The microspheres were injected in a volume of 3 ml over 30 s. Arterial reference blood was withdrawn from the aorta at a flow rate of 10 ml/min for 90 s. On termination of the experiment 1 g of tissue samples were isolated from the brain, the kidney, the liver, the spleen, the stomach and the proximal, mid- and distal parts of the jejunum. Organ blood flow was determined by means of the coloured microspheres content [8, 9, 10].
Near-infrared spectroscopy
Near-infrared spectroscopy NIRO 300 (Hamamatsu, Hamamatsu City) was used. TOI of the liver was computed with SRS. An inter-optode distance of 4 cm was used. TOI is calculated according to the diffusion equation as follows [1, 2]:
where k is the constant scattering contribution.
Mean arterial blood pressure (MABP), ECG, pulse rate and peripheral oxygen saturation were recorded in an analogue way by the data acquisition system Codas (Dataq Instruments, USA). Since the NIRS measurements are digital with a sampling rate of 6 Hz, they were converted to analogue signals with a sample-and-hold function before their introduction in the Codas system. The mean TOI was calculated over 1 min, just before the blood sample and before the injection of microspheres to avoid any interference.
Statistics
Statistica (Statsoft) was used. Repeated measures ANOVA test was used to assess the change in the different parameters between 33°C and 35°C and between 35°C and 37°C (steps 1–3). Paired t-tests were calculated to describe the effects of change in PaCO2 (step 4). The relationship between variables was assessed using Pearson’s correlation coefficients (mean, 95% C.I. and p value) over the total experiment. To correct for the repeated observations, we used the ANCOVA test [11].
Results
The total procedure was performed in six newborn piglets. The results for the total experiment are described in Table 1. Regarding the oxygenation parameters, we could not find a significant change in TOI or the mixed oxygen saturation during change in temperature or change in PaCO2. Regarding the organ flow, we found a decrease in intestinal blood flow at each step of the rewarming procedure and an increase in intestinal blood flow after the change in PaCO2. These changes, however, were not significant. No significant changes were found in PaO2, PaCO2, MABP or haemoglobin during the rewarming procedure. During the hypocapnia procedure no significant changes in PaO2, MABP or haemoglobin were found. Although no significant decrease in PaCO2 was seen over the whole group, ΔPCO2 was −10.8 mmHg (−6.7 to −4.8 mmHg).
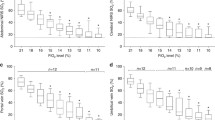
Table 2 shows the correlation of TOI with the different oxygenation parameters. TOI correlated well with the mixed venous saturation (r=0.85 and p<0.0001) and this remained significant after correction with ANCOVA. The correlation between TOI of the liver and the organ blood flows is also shown in Table 2. There was a positive correlation with the flow in the mid portion of the small bowel (r=0.57 and p=0.01) and this remained significant after correction with ANCOVA (Fig. 1). There was also a positive correlation with the blood flow in the distal ileum (r=0.72 and p=0.0005) and this remained significant after correction with ANCOVA. There was no significant correlation between TOI of the liver and temperature, PaCO2, MABP and haemoglobin after correction with ANCOVA.

The scatter plots of the relation between tissue oxygenation index and the distal ileal blood flow. Nineteen measurements were performed. The regression lines are shown on the graph. Pearson’s correlation coefficient was r=0.72 with p=0.0005 and, after correction with ANCOVA, p=0.03
Discussion
We found a positive correlation between TOI and mixed venous oxygen saturation, measured in the pulmonary artery. This confirms the studies of Schultz and Weiss, who described a good correlation between the TOI of the liver measured with NIRO 300 and the central venous oxygen saturation measured in the right atrium in children during cardiac catheterisation [3, 4].
The second hypothesis regarding the relation between TOI of the liver and the splanchnic circulation could not be confirmed. Only the blood flow delivered by the hepatic artery is measured with the coloured microspheres. The portal vein will not contain coloured microspheres because they are retained in the intestinal microcirculation. The absent correlation between hepatic arterial blood flow and TOI confirms the former NIRS studies on the liver as described by Tokuka et al. [12].
The third hypothesis regarding the relation with intestinal blood flow revealed a positive correlation between the blood flow in the distal ileum and the TOI of the liver. The start of oxygen supply dependence occurs earlier in the gut than in the rest of the body [13]. If there is an important decrease in oxygen delivery while oxygen consumption remains stable or decreases less, an increase in oxygen extraction is expected. This will first occur in the ileum because there is less autoregulation and the oxygen extraction is less effective compared with the stomach and the proximal jejunum [14, 15, 16]. The increase in oxygen extraction results in a decrease in venous mesenteric oxygenation and, consequently, a decrease in venous portal oxygenation. In this way, the measurement of TOI of the liver might be a good and early predictor of intestinal ischaemia. Further larger studies must be performed to confirm this relation before any clinical application, like using TOI of the liver as a trend monitoring for intestinal ischaemia, can be studied.
References
Matcher J, Kirkpatrick PJ, Nahid M, Cope M, Delpy DT (1995) Absolute quantification methods in tissue near infrared spectroscopy. Proc SPIE 2389:486–495
Suzuki S, Takasaki S, Ozaki T, Kobayashi Y (1999) A tissue oxygenation monitor using NIR spatially resolved spectroscopy. Proc SPIE 3597:582–592
Schulz G, Weiss M, Bauersfeld U, Teller J, Haensse D, Bucher HU, Baenziger O (2002) Liver tissue oxygenation as measured by near-infrared spectroscopy in the critically ill child in correlation with central venous oxygen saturation. Intensive Care Med 28:184–189
Weiss M, Schulz G, Fasnacht M, Balmer C, Fischer JE, Gerber AC, Bucher HU, Baenziger O (2002) Transcutaneously measured near-infrared spectroscopic liver tissue oxygenation does not correlate with hepatic venous oxygenation in children. Can J Anaesth 49:824–829
Teller J, Wolf M, Keel M, Bucher HU, Fanconi S, Baenziger O (2000) Can near infrared spectroscopy of the liver monitor tissue oxygenation? Eur J Pediatr 159:549
Gray H (1980) Gray’s anatomy. 36:763–765
Teller J, Schwendener K, Wolf M, Keel M, Bucher HU, Fanconi S, Baenziger O (2000) Continuous monitoring of liver oxygenation with near infrared spectroscopy during naso-gastric tube feeding in neonates. Schweiz Med Wochenschr 130:652–656
Kowallik P, Schulz R, Guth BD, Schade A, Paffhausen W, Gross R, Heusch G (1991) Measurement of regional myocardial blood flow with multiple colored microspheres. Circulation 83:974–982
Rudolph AM, Heymann MA (1967) The circulation of the fetus in utero. Methods for studying distribution of blood flow, cardiac output and organ blood flow. Circ Res 21:163–184
Wieland W, Wouters PF, Van Aken H, Flameng W (1993) Measurement of organ blood flow with coloured microspheres: a first time-saving improvement using automated spectrophotometry. Proceedings of computers in cardiology. pp 691–694
Bland JM, Altman DG (1995) Statistics notes. Calculating correlation coefficients with repeated observations: Part 1–correlation within subject. BMJ 310:446
Tokuka A, Tanaka A, Kitai T, Yanabu N, Mori S, Sato B, Tanaka K, Yamaoka Y, Hirao K (1994) Interrelationship of oxygen supply by hepatic artery and portal vein: rapid analysis of ischemia-reflow-induced changes in hepatic oxygenation in experimental and clinical subjects by tissue near-infrared spectroscopy. Eur Surg Res 26:342–352
Nelson DP, King CE, Dodd CL, Schumacker PT, Cain SM (1987) Systemic and intestinal limits of O2-extraction in the dog. J Appl Physiol 63:387–394
Buckley NM, Brazeau P, Frasier ID (1986) Intestinal and femoral blood flow autoregulation in developing swine. Biol Neonate 49:229–240
Nowicki PT, Miller CE (1988) Autoregulation in the developing postnatal intestinal circulation. Am J Physiol 254: G189–G193
Tao W, Zwischenberger JB, Nguyen TT, Vertrees RA, McDaniel LB, Nutt LK, Herndon DN, Kramer GC (1995) Gut mucosal ischemia during normothermic cardiopulmonary bypass results from blood flow redistribution and increased oxygen demand. J Thorac Cardiovasc Surg 110:819–828
Acknowledgements
The research of Gunnar Naulaers was supported by FWO: Clinical Doctoral Grant A6/5 – CM. D 11.354. The research of Sabine Van Huffel was supported by the Belgian Programme of Inter-university Poles of Attraction (IUAP Phase V-22) initiated by the Belgian State, Prime Minister’s Office, Federal Office for Scientific, Technical and Cultural Affairs, of the Concerted Research Action (GOA) projects of the Flemish Government MEFISTO-666 (Mathematical Engineering for Information and Communication Systems Technology) and of the IDO/02/009 project (KU Leuven).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Naulaers, G., Meyns, B., Miserez, M. et al. Measurement of the liver tissue oxygenation by near-infrared spectroscopy. Intensive Care Med 31, 138–141 (2005). https://doi.org/10.1007/s00134-004-2482-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2482-3