
Abstract
Objective
To determine the validity of the esophageal Doppler monitor (EDM) and echo-esophageal Doppler (Echo-ED) in measuring cardiac output in the critically ill.
Design
Systematic search of relevant international literature and data synthesis.
Search strategy
Literature search (1989–2003) using Ovid interface to Medline, Embase and Cochrane databases aimed at finding studies comparing EDM or Echo-ED cardiac output with that derived from simultaneous pulmonary artery thermodilution (PACTD) with Bland Altman measures of validity.
Patients
Critically ill adults in operating departments or intensive care units.
Data synthesis
Summary validity measures synthesized from Bland Altman analyses included pooled median bias and the median percentage of clinical agreement (PCA) derived from the limits of agreement.
Main results
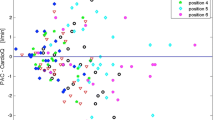
Eleven validation papers for EDM (21 studies) involving 314 patients and 2,400 paired measurements. The pooled median bias for PACTD versus EDM was 0.19 l/min (range −0.69 to 2.00 l/min) for cardiac output (16 studies), and 0.6% (range 0–2.3%) for changes in cardiac output (5 studies). The pooled median percentage of clinical agreement for PACTD versus EDM was 52% (interquartile range 42–69%) for cardiac output and 86% (interquartile range 55–93%) for changes in cardiac output. These differences in PCA were significant (p=0.03 Mann-Whitney) for bolus PACTD as the clinical “gold standard”. We found an insufficient number of studies (2 papers) to assess the validity of Echo-ED.
Conclusions
The esophageal Doppler monitor has high validity (no bias and high clinical agreement with pulmonary artery thermodilution) for monitoring changes in cardiac output.
Similar content being viewed by others

References
Pulmonary Artery Catheter Consensus Conference participants (1997) Pulmonary artery catheter consensus conference: consensus statement. Crit Care Med 25:910–924
Chaney JC, Derdak S (2002) Minimally invasive hemodynamic monitoring for the intensivist: current and emerging technology. Crit Care Med 30:2338–2345
Side C, Gosling R (1971) Non-surgical assessment of cardiac function. Nature 232:335–336
Singer M, Clarke J, Bennett ED (1989) Continuous hemodynamic monitoring by esophageal Doppler. Crit Care Med 17:447–452
Venn R, Rhodes A, Bennett ED (1999) The esophageal Doppler. In: Vincent JL (ed) Yearbook of Intensive Care and Emergency Medicine. Springer Verlag, Berlin, pp 482–493
Laupland KB, Bands CJ (2002) Utility of esophageal Doppler as a minimally invasive hemodynamic monitor: a review. Can J Anesth 49:393–401
Schmid ER, Spahn DR, Tornic M (1993) Reliability of a new generation transesophageal Doppler device for cardiac output monitoring. Anesth Analg 77:971–979
Bland MJ, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet I: 307–310
Colbert S, O’Hanlon DM, Duranteau J, Ecoffey C (1998) Cardiac output during liver transplantation. Can J Anesth 45:133–138
Valtier B, Cholley BP, Belot JP, de la Coussaye JE, Mateo J, Payen DM (1998) Noninvasive monitoring of cardiac output in critically ill patients using transesophageal Doppler. Am J Respir Crit Care Med 158:77–83
Nuan-Yen S, Chun-Jen H, Peishan T, Yung-Wei H, Yu-Chun H, Ching-Rong C (2002) Cardiac output measurement during cardiac surgery: esophageal Doppler versus pulmonary artery catheter. Acta Anaesthesiol Sin 40:127–123
Singer M, Bennett ED (1991) Noninvasive optimization of left ventricular filling using esophageal Doppler. Crit Care Med 19:1132–1137
Klotz KF, Klingsiek S, Singer M, Wenk H, Eleftheriadis S, Kuppe H, Schmucker P (1995) Continuous measurement of cardiac output during aortic cross-clamping by the oesophageal Doppler monitor ODM 1. Br J Anaesth 74:655–660
Keyl C, Rodig G, Lemberger P, Hobbhahn J (1996) A comparison of the use of transoesophageal Doppler and thermodilution techniques for cardiac output determination. Eur J Anaesth 13:136–142
Krishnamurthy B, McMurray TJ, McClean E (1997) The peri-operative use of oesophageal Doppler monitor in patients undergoing coronary artery revascularisation. A comparison with the continuous cardiac output monitor. Anaesth 52:624–629
Lefrant JY, Bruelle P, Aya AG, Saissi G, Dauzat M, de la Coussaye JE, Eledjam JJ (1998) Training is required to improve the reliability of esophageal Doppler to measure cardiac output in critically ill patients. Intensive Care Med 24:347–352
Baillard C, Cohen Y, Fosse JP, Karoubi P, Hoang P, Cupa M (1999) Haemodynamic measurements in critically ill patients: transoesophageal versus continuous thermodilution. Anaesth Intensive Care 27:33–37
Penny JA, Anthony J, Shennan AH, De Swiet M, Singer M (2000) A comparison of hemodynamic data derived by pulmonary artery flotation catheter and the esophageal Doppler monitor in pre-eclampsia. Am J Obstet Gynecol 183:658–661
Leather HA, Wouters PF (2001) Oesophageal Doppler monitoring overestimates cardiac output during lumbar epidural anaesthesia. Br J Anaesth 86:794–797
Jaeggi P, Hofer CK, Klaghofer R, Fodor P, Genoni M, Zollinger A (2003) Measurement of cardiac output after cardiac surgery by a new transesophageal Doppler device. J Cardiothorac Vasc Anesth 17:217–220
Le Tulzo Y, Belghith M, Seguin P, Dall’Ava J, Monchi M, Thomas R, Dhainaut JF (1996) Reproducibility of thermodilution cardiac output determination in critically ill patients: comparison between bolus and continuous method. J Clin Monit 12:379–385
Medin DL, Brown DT, Wesley R, Cunnion RE, Ognilbene FP (1998) Validation of continuous thermodilution cardiac output in critically ill patients with analysis of systematic errors. J Crit Care 13:184–189
Zollner C, Goetz AE, Weis M, Morstedt K, Pichler B, Lamm P, Kilger E, Haller M (2001) Continuous cardiac output measurements do not agree with conventional bolus thermodilution cardiac output determination. Can J Anesth 48:1143–1147
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dark, P.M., Singer, M. The validity of trans-esophageal Doppler ultrasonography as a measure of cardiac output in critically ill adults. Intensive Care Med 30, 2060–2066 (2004). https://doi.org/10.1007/s00134-004-2430-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2430-2