
Abstract
Background
Postoperative emergency agitation (EA) is a common problem. Dexmedetomidine and remifentanil may be used to prevent this problem. Our primary aim was to compare dexmedetomidine, remifentanil, and placebo with respect to their effectiveness in preventing postoperative EA.
Material and methods
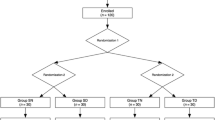
Ninety patients undergoing nasal surgery were randomized into three groups. The dexmedetomidine group (group D, n = 30) received dexmedetomidine infusion at a rate of 0.4 μg kg–1 h−1; the remifentanil group (group R, n = 30) received remifentanil infusion at a rate of 0.05 μg kg–1 min−1 from induction of anesthesia until extubation; and the control group (group S, n = 30) received a volume-matched normal saline infusion as a placebo. Propofol (1.5–2 mg kg−1) and fentanyl (1 μg kg−1) were used to initiate anesthesia, and desflurane was used to maintain anesthesia. The incidence of agitation, hemodynamic parameters, and recovery characteristics were evaluated during emergence.
Results
The incidence of EA was significantly higher in group S (46.7 %) compared with groups R and D (3.3 and 20 %, respectively; p < 0.001). The lowest incidence of EA was detected in group R (p = 0.046). Residual sedation in the post-anesthesia care unit (PACU) was similar in all groups (p = 0.947). The incidence of nausea or vomiting was significantly lower in group D than in groups R and S (p = 0.043). Administration of analgesics in the PACU was higher in group R than in groups S and D (p = 0.015).
Conclusion
Anesthetic maintenance with either remifentanil or dexmedetomidine infusion until extubation provided a more smooth and hemodynamically stable emergence, without complications after nasal surgery. While remifentanil was superior to dexmedetomidine with regard to avoiding EA, dexmedetomidine was more effective than remifentanil regarding vomiting and pain.
Zusammenfassung
Hintergrund
Unser vorrangiges Ziel war es, Dexmedetomidin, Remifentanil und Placebo im Hinblick auf ihre Wirksamkeit bei der Verhinderung postoperativer Erregungszustände zu vergleichen.
Methode
Neunzig Patienten, die sich einer Nasenoperation unterzogen hatten, wurden in 3 Gruppen eingeteilt. Die Dexmedetomidingruppe (Gruppe D) erhielt eine Dexmedetomidininfusion in einer Konzentration von 0,4 μg kg−1 h−1, die Remifentanilgruppe (Gruppe R) erhielt eine Remifentanilinfusion in einer Konzentration von 0,05 μg kg−1 min−1, beginnend mit der Narkoseeinleitung bis zur Extubation, und die Kontrollgruppe (Gruppe S) erhielt eine volumengleiche normale NaCl-Infusion als Placebo. Die Inzidenz der Agitation, hämodynamische Parameter und das Aufwachverhalten wurden ausgewertet.
Ergebnisse
Die Inzidenz postoperativer Erregungszustände war in der Gruppe S im Vergleich zu den Gruppen R und D (p = 0,000) signifikant höher. Die niedrigste Inzidenz wurde in der Gruppe R (p = 0,046) festgestellt. Die residuale Sedierung im Aufwachraum (AWR) war in allen Gruppen ähnlich (p = 0,947). Die Häufigkeit von Übelkeit oder Erbrechen war in Gruppe D deutlich niedriger als in der Gruppe R und S (p = 0,043). Die Verabreichung von Schmerzmitteln im AWR war in der Gruppe R höher als in den Gruppen S und D (p = 0,015).
Schlussfolgerung
Die Narkoseausleitung entweder mit Remifentanil oder Dexmedtomidininfusion bis zur Extubation ermöglicht eine ruhigere, hämodynamisch stabilere und komplikationsärmere Aufwachphase im Vergleich zu einer NaCl-Infusion nach einer Nasenoperation. Obwohl postoperative Erregungszustände unter Remifentanilinfusion seltener auftraten als unter Dexmedetomidininfusion, erwies sich Dexmedetomidin gegenüber Remifentanil als überlegen bezüglich postoperativem Erbrechen und Schmerz.


Similar content being viewed by others


Change history
26 April 2023
An Editorial Expression of Concern to this paper has been published: https://doi.org/10.1007/s00101-023-01294-0
20 December 2023
This article has been retracted. Please see the Retraction Notice for more detail: https://doi.org/10.1007/s00101-023-01373-2
References
Lepouse C, Lautner CA, Liu L, Gomis P, Leon A (2006) Emergence delirium in adults in the post-anaesthesia care unit. Br J Anaesth 96:747–753
Yu D, Chai W, Sun X, Yao L (2010) Emergence agitation in adults: risk factors in 2,000 patients. Can J Anaesth 57:843–848
Feldman MA, Patel A (2010) Anesthesia for eye, ear, nose and throat surgery. In: Miller RD (ed) Miller’s Anesthesia, Vol 2. Churchill Livingstone Elsevier, Philadelphia, pp 2368
Fairbanks DN (1986) Complications of nasal packing. Otolaryngol Head Neck Surg 94:412–415
Miller KA, Harkin CP, Bailey PL (1995) Postoperative tracheal extubation. Anesth Analg 80:149–172
Patel A, Davidson M, Tran MC et al (2010) Dexmedetomidine infusion for analgesia and prevention of emergence agitation in children with obstructive sleep apnea syndrome undergoing tonsillectomy and adenoidectomy. Anesth Analg 111:1004–1010
Tufanogullari B, White PF, Peixoto MP et al (2008) Dexmedetomidine infusion during laparoscopic bariatric surgery: the effect on recovery outcome variables. Anesth Analg 106:1741–1748
Shukry M, Clyde MC, Kalarickal PL, Ramadhyani U (2005) Does dexmedetomidine prevent emergence delirium in children after sevoflurane-based general anesthesia? Paediatr Anaesth 15:1098–1104
Guler G, Akin A, Tosun Z et al (2005) Single-dose dexmedetomidine reduces agitation and provides smooth extubation after pediatric adenotonsillectomy. Paediatr Anaesth 15:762–766
Blaudszun G, Lysakowski C, Elia N, Tramèr MR (2012) Effect of perioperative systemic α2 agonists on postoperative morphine consumption and pain intensity: systematic review and meta-analysis of randomized controlled trials. Anesthesiology 116:1312–1322
Hoy SM, Keating GM (2011) Dexmedetomidine: a review of its use for sedation in mechanically ventilated patients in an intensive care setting and for procedural sedation. Drugs 71:1481–1501
Patel SS, Spencer CM (1996) Remifentanil. Drugs 52:417–427
Guldbrand P, Berggren l, Brattebo G, Scandınavıan Crıtıcal Care Trıals Group et al (2004) Survey of routines for sedation of patients on controlled ventilation in Nordic intensive care units. Acta Anesthesiol Scand 48:944–950
Lauwers M, Camu F, Breivik H et al (1999) The safety and effectiveness of remifentanil as an adjuncy sedative for regional anesthesia. Anesth Analg 88:134–140
Dong YX, Meng LX, Wang Y et al (2010) The effect of remifentanil on the incidence of agitation on emergence from sevoflurane anaesthesia in children undergoing adenotonsillectomy. Anaesth Intensive Care 38:718–722
Na HS, Song IA, Hwang JW, Do SH, Oh AY et al (2013) Emergence agitation in children undergoing adenotonsillectomy: a comparison of sevoflurane vs. sevoflurane-remifentanil administration. Acta Anaesthesiol Scand 57:100–105
Kavalci G, Ethemoglu FB, Durukan P et al (2013) Comparison of the effects of dexmedetomidine and remiphentanil on emergence agitation after sevoflurane anesthesia in adults undergoing septoplasty operation: a randomized double-blind trial. Eur Rev Med Pharmacol Sci 17:3019–3023
Riker RR, Picard JT, Fraser GL (1999) Prospective evaluation of the Sedation-Agitation Scale for adult critically ill patients. Crit Care Med 27:1325–1329
Aldrete JA (1995) The postanesthesia recovery score revisited. J Clin Anesth 7:89
Kuratani N, Oi Y (2008) Greater incidence of emergence agitation in children after sevoflurane anesthesia as compared with halothane: a meta-analysis of randomized controlled trials. Anesthesiology 109:225–232
Sun L, Guo R, Sun L (2014) Dexmedetomidine for preventing sevoflurane-related emergence agitation in children: a meta-analysis of randomized controlled trials. Acta Anaesthesiol Scand 58:642–650
Kim SY, Kim JM, Lee JH et al (2013) Efficacy of intraoperative dexmedetomidine infusion on emergence agitation and quality of recovery after nasal surgery. Br J Anaesth 111:222–228
Cavaliere F, Antonelli M, Arcangeli A et al (2002) A low-dose remifentanil infusion is well tolerated for sedation in mechanically ventilated, critically-ill patients. Can J Anaesth 49:1088–1094
Ham SY, Kim JE, Park C et al (2014) Dexmedetomidine does not reduce emergence agitation in adults following orthognathic surgery. Acta Anaesthesiol Scand 58:955–960
Aouad MT, Al-Alami AA, Nasr VG et al (2009) The effect of low-dose remifentanil on responses to the endotracheal tube during emergence from general anesthesia. Anesth Analg 108:1157–1160
Mignat C, Wille U, Ziegler A (1995) Affinity profiles of morphine, codeine, dihydrocodeine and their glucuronides at opioid receptor subtypes. Life Sci 56:793–799
Cravero JP, Beach M, Thyr B et al (2003) The effect of small dose fentanyl on the emergence characteristics of pediatric patients after sevoflurane anesthesia without surgery. Anesth Analg 97:364–367
Weldon BC, Bell M, Craddock T (2004) The effect of caudal Analgesia on emergence agitation in children after sevoflurane versus halothane anesthesia. Anesth Analg 98:321–326
Guignard B, Bossard AE, Coste C et al (2000) Acute opioid tolerance: intraoperative remifentanil increases postoperative pain and morphine requirement. Anesthesiology 93:409–417
Choi HR, Cho JK, Lee S et al (2011) The effect of remifentanil versus N(2)O on postoperative pain and emergence agitation after pediatric tonsillectomy/adenoidectomy. Korean J Anesthesiol 61:148–153
Davis PJ, Finkel JC, Orr RJ, et al (2000) A randomized, double-blinded study of remifentanil versus fentanyl for tonsillectomy and adenoidectomy surgery in pediatric ambulatory surgical patients. Anesth Analg 90:863–871
Furst SR, Rodarte A (1994) Prophylactic antiemetic treatment with ondansetron in children undergoing tonsillectomy. Anesthesiology 81:799–803
Coda BA (2009) Opioids. In: Barash PG, Cullen BF, Stoelting RK, Cahalan MK, Stock MC (eds) Clinical anesthesia, 6th edn. Lippincott Williams & Wilkins, Philadelphia, pp 484–487
Herr DL, Sum-Ping ST, England M (2003) ICU sedation after coronary artery bypass graft surgery: dexmedetomidine-basedversus propofol-based sedation regimens. J Cardiothorac Vasc Anesth 17:576–584
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
R. Polat, K. Peker, I. Baran, G. Bumin Aydin, Ç. Topçu Gülöksüz, and A. Dönmez state that there are no conflicts of interest.
All studies on humans described in the present manuscript were carried out with the approval of the responsible ethics committee and in accordance with national law and the Helsinki Declaration of 1975 (in its current, revised form). Informed consent was obtained from all patients included in studies.
Additional information
This article has been retracted. Please see the retraction notice for more detail:https://doi.org/10.1007/s00101-023-01373-2
The article to which this update relates has been retracted. Please see the retraction notice for more detail: https://doi.org/10.1007/s00101-023-01373-2
About this article

Cite this article
Polat, R., Peker, K., Baran, I. et al. RETRACTED ARTICLE: Comparison between dexmedetomidine and remifentanil infusion in emergence agitation during recovery after nasal surgery. Anaesthesist 64, 740–746 (2015). https://doi.org/10.1007/s00101-015-0077-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00101-015-0077-8