
Abstract
Background
Reirradiation is a potentially useful option for many patients with recurrent cancer, aiming at cure or symptom palliation, depending on disease/recurrence type and stage. The purpose of this follow-up study to a previous review from 2016 was to summarize all recently published randomized trials. Points of interest again included identifcation of methodological strengths and weaknesses, practice-changing results, and open questions.
Material and methods
Systematic review of trials published between 2015 and February 2023.
Results
We reviewed 7 additional trials, most of which addressed reirradiation of head and neck or brain tumours. The median number of patients was 60. Mirroring the previous review, trial design, primary endpoints and statistical hypotheses varied widely. The updated results only impact on decision making for reirradiation of nasopharynx cancer and glioma. Patients with one of these diseases, as well as other head and neck cancers, may benefit from reirradiation-induced local control, e.g. in terms of progression-free survival. For the first time, hyperfractionated radiotherapy emerged as preferred option for recurrent, inoperable nasopharynx cancer. Despite better therapeutic ratio with hyperfractionation, serious toxicity remains a concern after high cumulative total doses. Randomized trials are still lacking for prostate cancer and other sites.
Conclusion
Multicentric randomized trials on reirradiation are feasible and continue to refine the current standard of care for recurrent disease after previous radiotherapy. Ongoing prospective studies such as the European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer (ESTRO-EORTC) observational cohort ReCare (NCT: NCT03818503) will further shape the clinical practice of reirradiation.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Throughout many decades of clinical research and radiobiological animal studies, reirradiation has evolved into a widely utilized treatment, e.g., for bone metastases, brain metastases, head and neck cancer, prostate cancer and other malignancies [1,2,3,4,5,6,7]. A recent consensus endorsed by the European Society for Radiotherapy and Oncology (ESTRO) and the European Organisation for Research and Treatment of Cancer (EORTC) aimed at a standardized classification of different forms of reirradiation and reporting [8]. The use of this classification in daily clinical practice and ongoing research will facilitate accurate understanding of the clinical implications of reirradiation and allow for cross-study comparisons. The consensus document was based on an adapted Delphi process and a systematic review of the literature. Reirradiation is a new course of radiotherapy, either to a previously irradiated volume (irrespective of concerns of toxicity) or where the cumulative dose raises concerns of toxicity [8]. Type 1 is a new course of radiotherapy that has geometrical overlap with the irradiated volume of previous courses (Fig. 1), and type 2 is a new course with concerns of toxicity from the cumulative doses but in which there is no overlap with the irradiated volume of previous courses, e.g., in the lungs. Repeat organ irradiation is a new course of radiotherapy to a previously irradiated organ but without overlap of the irradiated volumes and without concerns for toxicity from cumulative doses. As consistently reported, reirradiation might provide worthwhile clinical benefit in terms of symptom palliation, local tumor control and sometimes even cure after diagnosis of local or regional relapse or second primary tumours in a pretreated region. In parallel to single-arm studies, randomized clinical trials have been performed [9,10,11,12,13,14,15,16,17]. A previous review from 2016 evaluated the published randomized trials in order to identify methodological strengths and weaknesses, comment on the results, clinical implications and open questions, and advise on the planning of future trials [18]. The present updated review examines all additional publications up to February 2023.

Type 1 reirradiation is a new course of radiotherapy that has geometrical overlap with the irradiated volume of previous courses (left upper panel: prostate reirradiation to a biopsy-confirmed 68Ga-PSMA positron emission tomography (PET) positive (yellow arrow) relapse after previous external beam radiotherapy), and type 2 is a new course with concerns of toxicity from the cumulative doses but in which there is no overlap with the irradiated volume of previous courses (other panels, treatment planning computed tomography with fused PET in the same patient). Irradiating the single bone metastasis might increase the risk of bladder or bowel toxicity. In the absence of toxicity concerns, the term “repeat organ irradiation” is recommended. CTV clinical target volume: orange, PTV planning target volume: red, rectum: brown, bladder: yellow
Methods
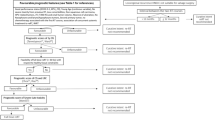
Inclusion was limited to trials published between 2015 and 2023, i.e. the recent literature. Trials were identified through systematic searches of the databases PubMed, Scopus and Web of Science by use of the key words ‘reirradiation’, ‘re-irradiation’, ‘repeat radiotherapy’, ‘radiation retreatment’ and ‘recurrent AND radiotherapy’ in February 2023. References from published trials and the consensus document were cross-checked.
Results and discussion
We identified and reviewed 7 randomized trials, which are presented in Table 1, together with 9 already discussed trials. Most of these new publications were related to head and neck tumours (two Chinese trials on nasopharynx cancer [19, 20] and one French trial on head and neck squamous cell cancer [21]) or glioblastoma/high-grade glioma (n = 3) [22,23,24]. The median number of patients in these 7 trials was 60. Three trials had a standard arm without reirradiation (surgery vs. reirradiation for nasopharynx cancer [19]; chemotherapy vs. fractionated stereotactic radiosurgery with chemotherapy for glioma [22]; bevacizumab vs. bevacizumab and reirradiation for glioblastoma [24]). The trials addressed important questions regarding dose/fractionation, combination with anti-cancer drugs, and toxicity.
Trial design, primary endpoints and statistical hypotheses varied widely. In three publications from our first review [18], information on these crucial components was missing to some extent. Now, no such missing data were identified. In line with the previous review, several trials were powered to detect substantial differences in overall survival or progression-free survival, i.e. ≥ 20%, which are uncommon in this setting. All reports provided sufficient details on inclusion and exclusion crtiteria allowing the readers to judge these quality criteria. However, the median length of follow-up was not reported in two of the publications [22, 23].
Nasopharynx cancer
Except for the landmark bone metastases trial from 2014, the randomized phase 3 trial by Liu et al. [19] represents the largest reirradiation study (n = 200). These researchers confirmed that salvage surgery (endoscopic nasopharyngectomy) is an important option for resectable recurrences, leading to improved 3‑year overall survival compared to intensity-modulated radiotherapy (IMRT; 86% versus 68%, p = 0.0015). Most patients had N0‑1 disease. Seventy-one (71%) of the 100 patients in the IMRT group received cisplatin-based chemotherapy. IMRT was not fully standardized regarding dose per fraction and total dose (60–70 Gy). A proportion of patients (> 30%) had received initial radiotherapy with less advanced techniques that often result in higher doses to critical organs at risk. In line with previous studies, reirradiation caused a relatively high rate of serious toxicity. The most common grade 3 or worse radiation-related late adverse event was pharyngeal mucositis (26% after IMRT). Five (5%) of the patients who underwent surgery and 20% of patients who underwent IMRT died due to late toxic effects specific to radiotherapy. Connecting the toxicity in the reirradiation arm to initial radiotherapy or trial radiotherapy was difficult due to the long-term nature of radiation-related toxicity. However, the fact that high-dose reirradiation may cause fatal toxicity is well-known from the literature [26,27,28].
A previous randomized trial in nasopharynx cancer had evaluated de-escalation of the equivalent dose (EQD2) for late responding normal tissues, while maintaining the same EQD2 for tumour cells [10]. This was accomplished by selecting a slightly hypofractionated experimental regimen, which was compared to a conventional regimen with 2‑Gy fractions and longer overall treatment time (Table 1). It was assumed that normal tissue sparing would result in less life-threatening toxicity and thus better overall survival, i.e. a better therapeutic ratio. Indeed, the results showed a 5-year overall survival rate of 44% versus 30%, but the difference was not statistically significant (p = 0.06) in this underpowered study. Serious toxicity was not uncommon and therefore, further EQD2 reduction has now been studied. Hyperfractionation was employed to mitigate toxicity, while maintaining the same overall treatment time [20]. Standard IMRT was identical to the previous study, i.e. 60 Gy in 27 fractions, while hyperfractionated IMRT featured 65 Gy in 54 fractions (2 fractions per day). Overall survival and toxicity were the primary endpoints in this 144-patient trial. Patients were not allowed to have radiation-induced complications grade ≥ 3 before reirradiation. Regarding outcomes, reduced grade 3 or worse late radiation-induced toxicity was observed in the hyperfractionation arm (34% versus 57%, p = 0.02), in line with radiobiological assumptions. Significant differences favouring hyperfractionated radiotherapy were seen in the general quality-of-life domains of global health status, role functioning, and social functioning, and in the symptom burden domains of pain, financial difficulties, and loss of appetite. Furthermore, 3‑year overall survival was better after hyperfractionation (75% versus 55%, p = 0.01). Efficacy was suboptimal, given that 49% of patients in the hyperfractionation group and 46% in the standard once-daily fractionation group had locoregional relapse. A possible strategy would be to moderately increase the dose per fraction in the hyperfractionation regimen and/or to add 1–2 additional days, resulting in dose escalation. However, this carries a risk of increasing fatal toxicity and leaving overall survival unchanged. Alternatively, assuming that not all recurrent tumours are sufficiently sensitive to further irradiation, incorporating other approaches such as drug treatment may be warranted [29].
Head and neck squamous cell cancer
A French group reported a phase 2 randomized multicentric trial comparing two regimens of reirradiation after salvage surgery: mono-fractionated radiotherapy with concomitant chemotherapy and hyperfractionated radiotherapy with cetuximab as experimental arm [21]. The primary endpoint was the comparison of the number of patients with a treatment interruption for more than 15 days, due to acute toxicity. Thus, size was limited to 60 patients. Inclusion criteria included, e.g., > 6 months between the initial course of radiotherapy and salvage surgery, sufficient healing for beginning reirradiation within 8 weeks of salvage surgery, age 18–75 years, WHO performance status (PS) 0–1, no severe sequelae of initial radiotherapy, and > 50% of recurrent tumor had received ≥ 50 Gy during previous irradiation. One arm employed the so-called Vokes protocol, i.e. 60 Gy in 11 weeks (6 cycles, with each cycle delivering 2 Gy/fraction, 5 days/week, with concomitant hydroxyurea (1.5 g/d orally) and continuous infusion fluorouracil (800 mg/m2/day), with 9‑day rest periods between cycles (split course)). In the radiobiologically more sound hyperfractionated radiotherapy arm, patients received a total dose of 60 Gy in 50 fractions, 1.2 Gy/fraction, 2 fractions/day, 5 days/week during 5 weeks. Cetuximab was initiated one week before radiotherapy at a loading dose of 400 mg/m2, followed by weekly 250 mg/m2 during radiotherapy. Similar rates of more than 15 days of treatment interruption due to toxicity were reported (n = 1 and 0, respectively, p = 0.49). Overall, toxicities and disease-free survival (DFS) were not different between the two arms. Thus, hyperfractionated reirradiation of 60 Gy/5 weeks with cetuximab was tolerable. The median DFS of 12 months was modest, however approximately 30% of patients remained progression-free at 4 years. Loco-regional recurrence was the main cause of death, again demonstrating that recurrent disease is difficult to control, both at first and subsequent relapse.
In a previous study, 130 patients who underwent salvage surgery were randomly assigned to receive reirradiation (60 Gy) combined with concomitant chemotherapy (5-FU and hydroxyurea) versus no adjuvant treatment [12]. A significant improvement with regard to the primary endpoint of loco-regional tumour control (hazard ratio (HR) 2.7; 95% confidence interval (CI) 1.7–4.5; p < 0.001) and DFS (HR 1.7; 95% CI 1.1–2.5; p = 0.01) was observed in those patients who were assigned to receive postoperative chemo-reirradiation compared to those who underwent surgery alone. However, this benefit in DFS did not translate into a significant improvement of overall survival. The gain in loco-regional tumour control and DFS was achieved at the cost of significantly higher rates of grade 3–4 late side effects (39% versus 10% at 2 years, respectively). Importantly, patients allocated to the wait-and-see arm could receive salvage chemo-reirradiation at the time of loco-regional recurrence after salvage surgery, which was the case in 25% of patients. This type of cross-over reduces the likelihood of improved overall survival. In the newer but smaller hyperfractionation study [21], 2/14 patients in that arm had grade 3–4 toxicity at 2 years (trismus and dysphagia), supporting the concept of hyperfractionation if one proceeds to postoperative reirradiation in selected cases. Based on the results of both studies, a wait-and-see policy may also be considered, in particular when patients suffer from continuous late toxicity from the first course of treatment.
Primary brain tumours
Bergman et al. performed a small, prematurely closed trial of fractionated stereotactic radiosurgery with chemotherapy versus chemotherapy alone for bevacizumab (BEV)-resistant high-grade glioma, largely glioblastoma [22]. Chemotherapy drugs were chosen at the discretion of the treating physician recommended by the tumor board. Patients were stratified by KPS (≤ 80 vs > 80). The primary endpoints were local tumour control at 2 months and PFS. It was assumed that the reirradiation group would have a local control rate of 40% compared to a 10% rate in the comparator group. A total dose of 32 Gy (4 fractions of 8 Gy) was prescribed to a gross tumour volume (GTV; range 3‑186 cc), defined as the T1-weighted contrast-enhancing lesion plus the area of diffusion-weighted imaging seen on the co-registered magnetic resonance imaging scans (MRI). A dose of 24 Gy was prescribed to a clinical target volume (CTV) defined as the area of the new or change in T2-weighted fluid-attenuated inversion recovery abnormality. Treatment was planned via a simultaneous integrated boost (SIB) technique. The dose was prescribed to the highest isodose line encompassing the CTV, which ranged from 50 to 95% of the maximum dose. Planning target volume (PTV) was equal to GTV or CTV, respectively. There was no limit to the maximum target volume. It was assumed that all critical structures had received the maximum point dose during initial external beam radiation treatment. The dose constraints from the American Association of Physicists in Medicine Task Group 101 (TG101) report of stereotactic body radiation therapy for 3‑fraction treatments were used [30]. Coverage to the 32 Gy volume was not compromised based on those constraints. The median time from initial diagnosis to enrollment was 20.5 months (range 7 to 268) and the median number of prior recurrences was 3 (range 2 to 6). The reirradiation group had an improved median PFS compared to BEV-based chemotherapy alone (5.1 months, 95% CI 4.1–6.2 vs 1.8 months, 95% CI 1.2–2.8; p < 0.001). The reirradiation group had a better overall survival compared to the BEV/chemotherapy only group, but this difference was not statistically significant (median overall survival: 7.2 months [95% CI 6.1–8.1] vs 4.8 months [95% CI 1.7–7.6]; p = 0.11). Reirradiation toxicity grade 3 included one patient each with headache, nausea/vomiting, new onset weakness, intratumoural hemorrhage, and seizure (no grade 4 or 5 toxicities). There were no documented cases of radionecrosis.
Lower reirradiation EQD2 was employed in the German ERGO2 trial, a randomized trial of calorie-restricted ketogenic diet and fasting in addition to reirradiation for malignant glioma, largely glioblastoma [23]. It included 50 patients and required KPS ≥ 60 and interval at least 6 months, among other criteria. Most patients had 5 or 10 fractions of reirradiation (5 fractions of 4 Gy (mainly), 10 fractions of 3.5 Gy). The authors assumed PFS at 6 months to increase from 0% to 30%. No significant difference was observed in PFS at 6 months: 20% vs. 16%, p = 0.7. Similar median overall survival was achived (10.9 vs. 9.5 months). During the dietray intervention phase until day 12, 9 adverse events (experimental arm: 4, standard diet (SD): 5) were reported. Three patients suffered from epileptic seizures. The other adverse events were headache, nausea, or possible epileptic seizures with short-lasting aphasia, which could not be categorized by the description from the patient. From day 12 until the first MRI follow-up after 1 month, 11 adverse events (experimental arm: 5, SD: 6) were reported, the majority of which were epileptic seizures. The publication did not comment on radionecrosis. In summary, ERGO2 demonstrated that this dietary intervention can be safely applied to patients with recurrent glioma.
The largest (n = 170) and thus most important recent trial was NRG Oncology/RTOG1205, a randomized phase 2 trial to determine whether BEV plus reirradiation (experimental arm) would improve survival (primary endpoint) compared with BEV alone (control arm) [24]. Patients were stratified by age (< 50 years vs ≥ 50 years), KPS (60 vs 70–80 vs 90–100), and recent re-resection. Inclusion criteria were modified after slow accrual to allow for patient enrollment with up to three relapses, a KPS of ≥ 60, and recurrent tumors ≤ 6 cm. Multifocal recurrence was no longer excluded, provided that the composite tumor volume was ≤ 6 cm. Reirradiation dose was 35 Gy in 10 fractions, using 3D conformal technique, IMRT or protons. The protocol defined certain organ-at-risk doses (planning organ-at-risk volumes, 3 mm margin) and acceptable variations. Optic nerves and chiasm (D0.3cc) were constrained to 20 Gy (acceptable variation: 25 Gy). The respective figures were 24 and 30 Gy for brain stem (D0.3cc). GTV was defined as enhancing tumour using computed tomography and/or MRI or postoperative resection cavity if no residual enhancing tumour was noted. A PTV expansion of at least 3 mm was used. BEV was administered at a dose of 10 mg/kg every 2 weeks until disease progression. Patients randomly assigned to the BEV and reirradiation arm received an initial induction BEV dose (day 1) followed by concurrent BEV and radiation at the next dose (day 14), and then once every 14 days until disease progression. The median survival for the control arm was 9.7 months (80% CI, 9.0 to 11.2) and 10.1 months (95% CI, 9.5 to 11.3) for the experimental arm (HR, 0.98; 80% CI, 0.79 to 1.23, p = 0.46). Twelve patients on the BEV arm received reirradiation as salvage therapy. Furthermore, some imbalances in baseline characteristics favoured the BEV arm. The only notable survival difference between arms was noted for the KPS 90–100 subgroup, in which the BEV/reirradiation arm showed improved survival (HR, 0.67; 95% CI, 0.40 to 1.13; p = 0.13). The median PFS for the control versus reirradiation arms was 3.8 versus 7.1 months, respectively (HR, 0.73; 95% CI, 0.53 to 1.00; p = 0.05). No delayed grade 3 or worse treatment-related central nervous system adverse events were reported. The authors discussed that optimal treatment for patients with recurrent glioblastoma remains controversial in the absence of improved survival. Their study confirmed meaningful improvement in PFS, including the 6‑month PFS rate, which patients may consider clinically beneficial. Quality-of-life was not evaluated. Treatment was safe and well-tolerated with no delayed brain toxicities. Therefore, reirradiation (the study regimen or fewer stereotactic fractions) remains a reasonable option especially for patients with small volume of recurrence and good KPS, as also reflected in a recent guideline [31].
Breast cancer
Schouten et al. reported a prematurely closed randomized phase 2 study of reirradiation and hyperthermia versus reirradiation and hyperthermia plus chemotherapy for locally recurrent breast cancer in previously irradiated areas not suitable for resection (n = 49, planned: 104, slow accrual) [25]. Concurrent hormonal therapy was allowed. Patients were stratified by size of recurrence (> 5 cm or ≤ 5 cm) and time interval between primary breast cancer and first recurrence (> 3 years or ≤ 3 years). The authors tried to detect an increase in the local control rate after 1 year from 54% in the standard treatment arm to 69% in the experimental arm (corresponding to a HR of 0.6). Originally, 32 Gy was given in 8 fractions of 4 Gy in 4 weeks, at 2 fractions per week (3 days in between the fractions). After January 2015, the radiotherapy schedule was changed to 46 Gy in 23 fractions of 2 Gy, at 5 fractions per week. Local microwave hyperthermia was delivered once a week, starting within 1 h after radiotherapy. Patients receiving the 32-Gy schedule were given four sessions of hyperthermia and patients receiving the 46-Gy schedule were given five sessions of hyperthermia, a modality with long track record [32, 33]. Patients were treated with weekly cisplatin 40 mg/m2 given intravenously for 4 courses, concurrent with hyperthermia. Approximately half of the patients had already been unsuccessfully treated for the current relapse with surgery, chemotherapy, hormonal therapy or trastuzumab. Local (infield) progression-free rate at 1 year was high in both arms, 81.5% in the standard arm and 88% in the combined arm. About 60% per arm achieved a complete response. With or without cisplatin, most patients had subsequent local control until last follow-up or death. No significant difference regarding any endpoint was observed. One patient in the standard arm died due to a necrotizing thoracic wall defect in the radiated area 3 months after treatment. We could not identify randomized trials on repeat breast-conserving surgery with reirradiation, a concept gaining increasing acceptance in well-selected patients [34].
Summary and conclusions
The objective of this follow-up study was to review all recently published randomized trials in order to identify methodological strengths and weaknesses, comment on the results and open questions, and highlight the role of the upcoming Recare trial in collecting cumulative dose distributions through a new cohort within the E2-RADIatE platform managed by the EORTC [8]. By adhering to the new consensus for trial reporting, the authors of future reirradiation publications can improve clinical practice and our understanding of dose-response relationships. Important findings from the current review include that many trials failed to recruite as anticipated, resulting in premature closure or major protocol changes introducing heterogeneity, and eventually small group size. Nevertheless, several adequately designed, conducted and reported trials confirm again that high-level evidence can be generated in the field of reirradiation. Multi-institutional collaboration is encouraged to complete sufficiently large trials. The trials with relatively long median follow-up and high cumulative total doses confirmed that serious toxicity remains a concern, and that curative reirradiation can either prevent or cause a fatal outcome. Hyperfractionation improves the therapeutic ratio in the scenarios reviewed here. For many other clinical scenarios where reirradiation is offered by many institutions, randomized trials are still lacking, e.g., prostate cancer [35]. Published guidelines and consensus recommendations may guide decision-making [29, 31, 34,35,36,37]. Advanced technologies are helpful in creating highly conformal dose distributions, making us wonder about the potential of hyperfractionated proton or carbon-ion beam reirradiation. Few of the present studies published organ-at-risk dose constraints. Attempts to correlate toxicity with administered dose were lacking. This knowledge gap will hopefully be closed through the international Recare study, aiming at image fusion and co-registration to judge the cumulative dose distributions.
References
Cozzi S, Finocchi Ghersi S, Bardoscia L et al (2023) Linac-based stereotactic salvage reirradiation for intraprostatic prostate cancer recurrence: toxicity and outcomes. Strahlenther Onkol 199:554–564
Pontoriero A, Lillo S, Caravatta L et al (2021) Cumulative dose, toxicity, and outcomes of spinal metastases re-irradiation: Systematic review on behalf of the Re-Irradiation Working Group of the Italian Association of Radiotherapy and Clinical Oncology (AIRO). Strahlenther Onkol 197:369–384
Boustani J, Ruffier A, Moya-Plana A et al (2021) Long-term outcomes and safety after reirradiation in locally recurrent nasopharyngeal carcinoma in a non-endemic area. Strahlenther Onkol 197:188–197
Baehr A, Trog D, Oertel M et al (2020) Re-irradiation for recurrent glioblastoma multiforme: a critical comparison of different concepts. Strahlenther Onkol 196:457–464
Nieder C, Mannsåker B, Yobuta R et al (2020) Provider decision regret‑a useful method for analysis of palliative thoracic re-irradiation for lung cancer? Strahlenther Onkol 196:315–324
Schlampp I, Rieber J, Adeberg S et al (2019) Re-irradiation in locally recurrent lung cancer patients. Strahlenther Onkol 195:725–733
Nieder C, Andratschke NH, Grosu AL (2013) Increasing frequency of reirradiation studies in radiation oncology: systematic review of highly cited articles. Am J Cancer Res 3:152–158
Andratschke N, Willmann J, Appelt AL et al (2022) European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer consensus on re-irradiation: definition, reporting, and clinical decision making. Lancet Oncol 23:e469–e478 (Erratum in: Lancet Oncol 2022;23:e492)
Li JC, Hu CS, Jiang GL et al (2006) Dose escalation of three-dimensional conformal radiotherapy for locally recurrent nasopharyngeal carcinoma: a prospective randomised study. Clin Oncol (R Coll Radiol) 18:293–299
Tian YM, Zhao C, Guo Y et al (2014) Effect of total dose and fraction size on survival of patients with locally recurrent nasopharyngeal carcinoma treated with intensity-modulated radiotherapy: A phase 2, single-center, randomized controlled trial. Cancer 120:3502–3509
Guan Y, Liu S, Wang HY, Guo Y et al (2016) Long-term outcomes of a phase II randomized controlled trial comparing intensity-modulated radiotherapy with or without weekly cisplatin for the treatment of locally recurrent nasopharyngeal carcinoma. Chin J Cancer 35:20
Janot F, de Raucourt D, Benhamou E et al (2008) Randomized trial of postoperative reirradiation combined with chemotherapy after salvage surgery compared with salvage surgery alone in head and neck carcinoma. J Clin Oncol 26:5518–5523
Tortochaux J, Tao Y, Tournay E et al (2011) Randomized phase III trial (GORTEC 98-03) comparing re-irradiation plus chemotherapy versus methotrexate in patients with recurrent or a second primary head and neck squamous cell carcinoma, treated with a palliative intent. Radiother Oncol 100:70–75
Rudžianskas V, Inčiūra A, Vaitkus S et al (2014) Reirradiation for patients with recurrence head and neck squamous cell carcinoma: a single-institution comparative study. Medicina (Kaunas) 50:92–99
Chow E, van der Linden YM, Roos D et al (2014) A randomized trial of single and multiple fractions of repeat radiation for painful bone metastases. Lancet Oncol 15:164–171
Wick W, Fricke H, Junge K et al (2014) A phase II, randomized, study of weekly APG101+reirradiation versus reirradiation in progressive glioblastoma. Clin Cancer Res 20:6304–6313
Kouloulias VE, Plataniotis GA, Kouvaris JR et al (2003) Re-irradiation in conjunction with liposomal doxorubicin for the treatment of skin metastases of recurrent breast cancer: a radiobiological approach and 2 year of follow-up. Cancer Lett 193:33–40
Nieder C, Langendijk JA, Guckenberger M et al (2016) Prospective randomized clinical studies involving reirradiation: Lessons learned. Strahlenther Onkol 192:679–686
Liu YP, Wen YH, Tang J et al (2021) Endoscopic surgery compared with intensity-modulated radiotherapy in resectable locally recurrent nasopharyngeal carcinoma: a multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Oncol 22:381–390
You R, Liu YP, Xie YL et al (2023) Hyperfractionation compared with standard fractionation in intensity-modulated radiotherapy for patients with locally advanced recurrent nasopharyngeal carcinoma: a multicentre, randomised, open-label, phase 3 trial. Lancet 401(10380):917–927
Tao Y, Faivre L, Laprie A et al (2018) Randomized trial comparing two methods of re-irradiation after salvage surgery in head and neck squamous cell carcinoma: Once daily split-course radiotherapy with concomitant chemotherapy or twice daily radiotherapy with cetuximab. Radiother Oncol 128:467–471
Bergman D, Modh A, Schultz L et al (2020) Randomized prospective trial of fractionated stereotactic radiosurgery with chemotherapy versus chemotherapy alone for bevacizumab-resistant high-grade glioma. J Neurooncol 148:353–361
Voss M, Wagner M, von Mettenheim N et al (2020) ERGO2: A prospective, randomized trial of calorie-restricted ketogenic diet and fasting in addition to reirradiation for malignant glioma. Int J Radiat Oncol Biol Phys 108:987–995
Tsien CI, Pugh SL, Dicker AP et al (2023) NRG Oncology/RTOG1205: A randomized phase II trial of concurrent bevacizumab and reirradiation versus bevacizumab alone as treatment for recurrent glioblastoma. J Clin Oncol 41:1285–1295
Schouten D, van Os R, Westermann AM et al (2022) A randomized phase-II study of reirradiation and hyperthermia versus reirradiation and hyperthermia plus chemotherapy for locally recurrent breast cancer in previously irradiated area. Acta Oncol 61:441–448
Spencer SA, Harris J, Wheeler RH et al (2001) RTOG 96-10: Reirradiation with concurrent hydroxyurea and 5‑fluorouracil in patients with squamous cell cancer of the head and neck. Int J Radiat Oncol Biol Phys 51:1299–1304
Langer CJ, Harris J, Horwitz EM et al (2007) Phase II study of low-dose paclitaxel and cisplatin in combination with split-course concomitant twice-daily reirradiation in recurrent squamous cell carcinoma of the head and neck: Results of Radiation Therapy Oncology Group protocol 9911. J Clin Oncol 25:4800–4805
Nieder C, Langendijk JA, Guckenberger M et al (2017) Preserving the legacy of reirradiation: A narrative review of historical publications. Adv Radiat Oncol 2:176–182
Ng WT, Soong YL, Ahn YC et al (2021) International recommendations on reirradiation by intensity modulated radiation therapy for locally recurrent nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys 110:682–695
Benedict SH, Yenice KM, Followill D et al (2010) Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys 37:4078–4101
Ziu M, Goyal S, Olson JJ (2022) Congress of Neurological Surgeons systematic review and evidence-based guidelines update on the role of radiation therapy in the management of progressive and recurrent glioblastoma in adults. J Neurooncol 158:255–264
Datta NR, Puric E, Klingbiel D et al (2016) Hyperthermia and radiation therapy in locoregional recurrent breast cancers: A systematic review and meta-analysis. Int J Radiat Oncol Biol Phys 94:1073–1087
Emami B, Scott C, Perez CA et al (1996) Phase III study of interstitial thermoradiotherapy compared with interstitial radiotherapy alone in the treatment of recurrent or persistent human tumors: A prospectively controlled randomized study by the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 34:1097–1104
Bottero M, Borzillo V, Pergolizzi S et al (2021) The Italian Association of Radiotherapy and Oncology recommendation for breast tumor recurrence: grades of recommendation, assessment, development and evaluation criteria. J Breast Cancer 24:241–252
Jereczek-Fossa BA, Marvaso G, Zaffaroni M et al (2021) Salvage stereotactic body radiotherapy (SBRT) for intraprostatic relapse after prostate cancer radiotherapy: An ESTRO ACROP Delphi consensus. Cancer Treat Rev 98:102206 (on the behalf of the European Society for Radiotherapy, Oncology Advisory Committee on Radiation Oncology Practice (ESTRO ACROP))
Harms W, Budach W, Dunst J et al (2016) Breast Cancer Expert Panel of the German Society of Radiation Oncology (DEGRO). DEGRO practical guidelines for radiotherapy of breast cancer VI: therapy of locoregional breast cancer recurrences. Strahlenther Onkol 192:199–208
Embring A, Blomstrand M, Asklid A et al (2023) Re-irradiation in paediatric tumours of the central nervous system: National guidelines from the Swedish workgroup of paediatric radiotherapy. Clin Oncol (r Coll Radiol). https://doi.org/10.1016/j.clon.2023.05.007
Funding
Open access funding provided by UiT The Arctic University of Norway (incl University Hospital of North Norway)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
C. Nieder, J. Willmann and N.H. Andratschke declare that they have no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nieder, C., Willmann, J. & Andratschke, N.H. Prospective randomized clinical studies involving reirradiation: update of a systematic review. Strahlenther Onkol 199, 787–797 (2023). https://doi.org/10.1007/s00066-023-02118-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-023-02118-1