
Abstract
Background
The goal of this study was to evaluate accelerated radiotherapy with and without temozolomide (TMZ) for glioblastoma multiforme (GBM).
Methods
This retrospective analysis evaluated 86 patients with histologically proven GBM who were treated with accelerated radiotherapy of 1.8 Gy twice daily to a total dose of 54 Gy within 3 weeks. Median age was 62 years and median Karnofsky index was 90. A total of 41 patients received radiotherapy only from 2002–2005 and 45 patients were treated with TMZ concomitantly and after radiotherapy from 2005–2007.
Results
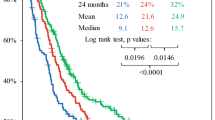
Median overall survival (OS) was 12.5 months and 2-year OS was 15.4%. Patient characteristics were well balanced between the two groups except for better performance status (p = 0.05) and higher frequency of retreatment for the first recurrence (p = 0.02) in the TMZ group. Age at diagnosis (HR 2.83) and treatment with TMZ (HR 0.60) were correlated with OS in the multivariate analysis: treatment with and without TMZ resulted in median OS of 16 months and 11.3 months, respectively. Hematological toxicity grade > II was observed in 2/45 patients and 5/37 patients during simultaneous radiochemotherapy and adjuvant TMZ.
Conclusion
TMZ added to accelerated radiotherapy for GBM resulted in prolonged overall survival with low rates of severe hematological toxicity.
Zusammenfassung
Hintergrund
Untersucht wurde die Behandlung des Glioblastoma multiforme (GBM) mittels akzelerierter Radiotherapie mit und ohne Temozolomid-(TMZ-)Chemotherapie.
Methodik
In dieser retrospektiven Auswertung wurden 86 Patienten mit histologisch gesichertem GBM erfasst, die mittels akzelerierter Strahlentherapie (zweimal täglich 1,8 Gy bis zu einer Gesamtdosis von 54 Gy in drei Wochen) behandelt wurden. Das mediane Alter war 62 Jahre, und der mediane Karnofsky-Index betrug 90. Im Zeitraum 2002–2005 wurden 41 Patienten mit alleiniger Strahlentherapie behandelt; im Zeitraum 2005–2007 erfolgte bei 45 Patienten zusätzlich zur Radiotherapie die simultane und adjuvante Gabe von TMZ.
Ergebnisse
Das mediane Überleben in der Gesamtkohorte betrug 12,5 Monate und das Zweijahresüberleben 15,4 %. Die Patienten- und Behandlungscharakteristika waren zwischen den beiden Gruppen ausgeglichen bis auf einen besseren Allgemeinzustand (p = 0,05) und eine höhere Rate an Rebehandlung beim ersten Rezidiv (p = 0,02) in der TMZ-Gruppe. Alter bei Diagnosestellung (HR 2,83) und Therapie mit TMZ (HR 0,60) waren in der multivariaten Analyse mit dem Gesamtüberleben korreliert. Das mediane Gesamtüberleben betrug 16 Monate und 11,3 Monate bei Therapie mit bzw. ohne TMZ. Hämatologische Toxizitäten Grad > II wurde bei 2/45 Patienten und 5/37 während Radiochemotherapie bzw. während adjuvanter TMZ-Therapie beobachtet.
Schlussfolgerungen
TMZ verbesserte im Kontext der akzelerierten Strahlentherapie das Gesamtüberleben bei gleichzeitig günstigem Toxizitätsprofil.
Similar content being viewed by others
References
Bleehen NM, Stenning SP. A Medical Research Council trial of two radiotherapy doses in the treatment of grades 3 and 4 astrocytoma. The Medical Research Council Brain Tumour Working Party. Br J Cancer 1991;64:769–774.
Brada M, Sharpe G, Rajan B et al. Modifying radical radiotherapy in high grade gliomas; shortening the treatment time through acceleration. Int J Radiat Oncol Biol Phys 1999;43:287–292.
Cho KH, Hall WA, Gerbi BJ et al. Single dose versus fractionated stereotactic radiotherapy for recurrent high-grade gliomas. Int J Radiat Oncol Biol Phys 1999;45:1133–1141.
Combs SE, Bischof M, Welzel T et al. Radiochemotherapy with temozolomide as re-irradiation using high precision fractionated stereotactic radiotherapy (FSRT) in patients with recurrent gliomas. J Neurooncol 2008;89:205–210.
Combs SE, Wagner J, Bischof M et al. Radiochemotherapy in patients with primary glioblastoma comparing two temozolomide dose regimens. Int J Radiat Oncol Biol Phys 2008;71:999–1005.
Do V, Gebski V, Barton MB. The effect of waiting for radiotherapy for grade III/IV gliomas. Radiother Oncol 2000;57:131–136.
Fabrini MG, Perrone F, De Franco L et al. Perioperative high-dose-rate brachytherapy in the treatment of recurrent malignant gliomas. Strahlenther Onkol 2009;185:524–529.
Fokas E, Wacker U, Gross MW et al. Hypofractionated stereotactic reirradiation of recurrent glioblastomas: a beneficial treatment option after high-dose radiotherapy? Strahlenther Onkol 2009;185:235–240.
Genc M, Zorlu AF, Atahan IL. Accelerated hyperfractionated radiotherapy in supratentorial malignant astrocytomas. Radiother Oncol 2000;56:233–238.
Gutin PH, Iwamoto FM, Beal K et al. Safety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomas. Int J Radiat Oncol Biol Phys 2009;75:156–163.
Hegi ME, Diserens AC, Gorlia T et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med 2005;352:997–1003.
Iliadis G, Selviaridis P, Kalogera-Fountzila A et al. The importance of tumor volume in the prognosis of patients with glioblastoma: comparison of computerized volumetry and geometric models. Strahlenther Onkol 2009;185:743–750.
Irwin C, Hunn M, Purdie G et al. Delay in radiotherapy shortens survival in patients with high grade glioma. J Neurooncol 2007;85:339–343.
Lai R, Hershman DL, Doan T, et al. The timing of cranial radiation in elderly patients with newly diagnosed glioblastoma multiforme. Neuro Oncol 2010;12:190–198.
Leitzen C, Schild HH, Bungart B et al. Prediction of clinical course of glioblastomas by MRI during radiotherapy. Strahlenther Onkol 2010;186:681–686.
Lutterbach J, Weigel P, Guttenberger R et al. Accelerated hyperfractionated radiotherapy in 149 patients with glioblastoma multiforme. Radiother Oncol 1999;53:49–52.
Matuschek C, Bolke E, Nawatny J et al. Bevacizumab as a treatment option for radiation-induced cerebral necrosis. Strahlenther Onkol 2011;187:135–139.
Nieder C, Andratschke N, Wiedenmann N et al. Radiotherapy for high-grade gliomas. Does altered fractionation improve the outcome? Strahlenther Onkol 2004;180:401–407.
Nieder C, Nestle U, Ketter R et al. Hyperfractionated and accelerated-hyper-fractionated radiotherapy for glioblastoma multiforme. Radiat Oncol Investig 1999;7:36–41.
Phillips C, Guiney M, Smith J et al. A randomized trial comparing 35Gy in ten fractions with 60Gy in 30 fractions of cerebral irradiation for glioblastoma multiforme and older patients with anaplastic astrocytoma. Radiother Oncol 2003;68:23–26.
Prados MD, Wara WM, Sneed PK et al. Phase III trial of accelerated hyperfractionation with or without difluromethylornithine (DFMO) versus standard fractionated radiotherapy with or without DFMO for newly diagnosed patients with glioblastoma multiforme. Int J Radiat Oncol Biol Phys 2001;49:71–77.
Roa W, Brasher PM, Bauman G et al. Abbreviated course of radiation therapy in older patients with glioblastoma multiforme: a prospective randomized clinical trial. J Clin Oncol 2004;22:1583–1588.
Roldan GB, Scott JN, McIntyre JB et al. Population-based study of pseudoprogression after chemoradiotherapy in GBM. Can J Neurol Sci 2009;36:617–622.
Sanghera P, Perry J, Sahgal A et al. Pseudoprogression following chemoradiotherapy for glioblastoma multiforme. Can J Neurol Sci 2010;37:36–42.
Schwer AL, Kavanagh BD, McCammon R et al. Radiographic and histopathologic observations after combined EGFR inhibition and hypofractionated stereotactic radiosurgery in patients with recurrent malignant gliomas. Int J Radiat Oncol Biol Phys 2009;73:352–357.
Shibamoto Y, Nishimura Y, Tsutsui K et al. Comparison of accelerated hyperfractionated radiotherapy and conventional radiotherapy for supratentorial malignant glioma. Jpn J Clin Oncol 1997;27:31–36.
Stupp R, Hegi ME, Mason WP et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 2009;10:459–466.
Vordermark D, Kolbl O, Ruprecht K et al. Hypofractionated stereotactic re-irradiation: treatment option in recurrent malignant glioma. BMC Cancer 2005;5:55.
Voynov G, Kaufman S, Hong T et al. Treatment of recurrent malignant gliomas with stereotactic intensity modulated radiation therapy. Am J Clin Oncol 2002;25:606–611.
Walker MD, Strike TA Sheline GE An analysis of dose-effect relationship in the radiotherapy of malignant gliomas. Int J Radiat Oncol Biol Phys 1979;5:1725–1731.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guckenberger, M., Mayer, M., Buttmann, M. et al. Prolonged survival when temozolomide is added to accelerated radiotherapy for glioblastoma multiforme. Strahlenther Onkol 187, 548–554 (2011). https://doi.org/10.1007/s00066-011-2242-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-011-2242-6