
Abstract
Purpose:
The optimal dose for salvage radiotherapy (SRT) after radical prostatectomy (RP) is still not defined. It should be at least 66 Gy. In the present study, the suitability of PSA regression as a selection criterion for an SRT dose escalation to 70.2 Gy was examined.
Patients and Methods:
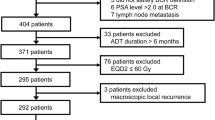
Between 1997 and 2007, 301 prostate cancer patients received SRT after RP at the Charité – University Medicine Berlin, Campus Benjamin Franklin. None of the patients had antihormone therapy prior to SRT. A total of 234 patients received 66.6 Gy. From 2002 on, 67 patients with a PSA decrease during SRT were irradiated with 70.2 Gy. The influence of this selection and dose escalation on freedom from biochemical progression (bNED) was analyzed.
Results:
The median follow-up of the whole group was 30 months, the median pre-SRT PSA was 0.28 ng/ml. Of the patients, 27% (82/301) developed biochemical progression, 31% from the 66.6 Gy cohort (73/292) and 13% from the 70.2 Gy cohort (9/67) (p = 0.01). The calculated 2-years bNED was 74% for the whole group, 88% vs. 71% after 70.2 Gy and 66.6 Gy, respectively (p = 0.01). In a multivariate analysis, the total dose (p = 0.017), the re-achievement of an undetectable PSA after SRT (p = 0.005), and the infiltration of the seminal vesicles (p = 0.049) were independent parameters of bNED.
Conclusion:
Our analysis suggests that patient selection during SRT for a dose escalation to 70.2 Gy can improve the freedom from biochemical progression in patients with SRT after RP.
Zusammenfassung
Ziel:
Die optimale Dosis der Salvage-Strahlentherapie (SRT) nach radikaler Prostatektomie (RP) ist derzeit nicht definiert. Sie sollte mindestens 66 Gy betragen. In der vorliegenden Arbeit wird die Bedeutung des PSA-Abfalls unter laufender SRT als Selektionskriterium für eine Dosiserhöhung auf 70,2 Gy untersucht.
Patienten und Methode:
Zwischen 1997 und 2007 wurden 301 Patienten mit Prostatakarzinom nach radikaler Prostatektomie an der Charité Universitätsmedizin, Campus Benjamin Franklin, Berlin, einer SRT unterzogen. Kein Patient hatte eine antihormo-nelle Therapie vor der SRT. 234 Patienten erhielten eine SRT-Dosis von 66,6 Gy. Seit 2002 wurden 67 Patienten mit einem PSA-Abfall unter SRT mit einer erhöhten Gesamtdosis von 70,2 Gy bestrahlt. Der Einfluss dieser Selektion mit der erhöhten Gesamtdosis auf die biochemische Progressionsfreiheit (bNED) nach SRT wird analysiert.
Ergebnisse:
Die mediane Nachbeobachtungszeit für die Gesamtgruppe war 30 Monate, der mediane Prä-SRT-PSA war 0,28 ng/ml. 27% (82/301) der Patienten entwickelten eine biochemische Progression, 31% in der Behandlungsgruppe mit 66,6 Gy (73/292) und 13% in der Gruppe mit 70,2 Gy (9/67), (p = 0,01). Die berechnete bNED nach 2 Jahren war 74% für die Gesamtgruppe und 88% vs. 71% bei 70,2 Gy bzw. 66.6 Gy (p = 0,01). In der multivariaten Analyse zeigten sich die Gesamtdosis (p = 0,017) das Wiedererreichen des PSA-Null-Bereichs nach SRT (p = 0,005) und die Samenblaseninfiltration (p = 0,049) als unabhängige Einflussfaktoren auf die bNED.
Schlussfolgerung:
Unsere Untersuchungen weisen darauf hin, dass eine Patientenselektion unter SRT in Verbindung mit einer Dosiseskalation auf 70,2 Gy die biochemische Progressionsfreiheit von Patienten mit SRT nach RP verbessern kann.
Similar content being viewed by others


References
Anscher MS, Clough R, Dodge R. Radiotherapy for a rising prostate-specific antigen after radical prostatectomy: the first 10 years. Int J Radiat Oncol Biol Phys 2000;48:369–375.
Bernard JR, Jr., Buskirk SJ, Heckman MG et al. Salvage radiotherapy for rising prostate-specific antigen levels after radical prostatectomy for prostate cancer: dose-response analysis. Int J Radiat Oncol Biol Phys 2010;76:735–740.
Bohrer M, Schroder P, Welzel G et al. Reduced rectal toxicity with ultrasound-based image guided radiotherapy using BAT (B-mode acquisition and targeting system) for prostate cancer. Strahlenther Onkol 2008;184:674–678.
Bolla M, van Poppel H, Collette L et al. Postoperative radiotherapy after radical prostatectomy: a randomised controlled trial (EORTC trial 22911). Lancet 2005;366:572–578.
Bottke D, de Reijke TM, Bartkowiak D et al. Salvage radiotherapy in patients with persisting/rising PSA after radical prostatectomy for prostate cancer. Eur J Cancer 2009;45Suppl 1:148–157.
Bottke D, Wiegel T. Radiotherapy and Prostate Cancer: Quo Vadis? Eur Urol 2010;9Suppl:394–400.
Chawla AK, Thakral HK, Zietman AL et al. Salvage radiotherapy after radical prostatectomy for prostate adenocarcinoma: analysis of efficacy and prognostic factors. Urology 2002;59:726–731.
Chun FK, Graefen M, Zacharias M et al. Anatomic radical retropubic prostatectomy-long-term recurrence-free survival rates for localized prostate cancer. World J Urol 2006;24:273–280.
Coen JJ, Zietman AL, Thakral H et al. Radical radiation for localized prostate cancer: local persistence of disease results in a late wave of metastases. J Clin Oncol 2002;20:3199–3205.
Cox DR. Regression models and life tables. J R Stat Soc 1972;(B)34:187–202.
Do T, Parker RG, Do C et al. Salvage radiotherapy for biochemical and clinical failures following radical prostatectomy. Cancer J Sci Am 1998;4:324–330.
Guckenberger M, Ok S, Polat B et al. Toxicity after intensity-modulated, image-guided radiotherapy for prostate cancer. Strahlenther Onkol 2010;186:535–543.
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Amer Stat Ass 1958;53:457–462.
King CR, Spiotto MT. Improved outcomes with higher doses for salvage radiotherapy after prostatectomy. Int J Radiat Oncol Biol Phys 2008;71:23–27.
Macdonald OK, Schild SE, Vora SA et al. Radiotherapy for men with isolated increase in serum prostate specific antigen after radical prostatectomy. J Urol 2003;170:1833–1837.
Morris MM, Dallow KC, Zietman AL et al. Adjuvant and salvage irradiation following radical prostatectomy for prostate cancer. Int J Radiat Oncol Biol Phys 1997;38:731–736.
Pazona JF, Han M, Hawkins SA et al. Salvage radiation therapy for prostate specific antigen progression following radical prostatectomy: 10-year outcome estimates. J Urol 2005;174:1282–1286.
Pinto F, Prayer-Galetti T, Gardiman M et al. Clinical and pathological characteristics of patients presenting with biochemical progression after radical retropubic prostatectomy for pathologically organ-confined prostate cancer. Urol Int 2006;76:202–208.
Pisansky TM, Kozelsky TF, Myers RP et al. Radiotherapy for isolated serum prostate specific antigen elevation after prostatectomy for prostate cancer. J Urol 2000;163:845–850.
Roehl KA, Han M, Ramos CG et al. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3,478 consecutive patients: long-term results. J Urol 2004;172:910–914.
Sautter-Bihl ML, Sedlmayer F, Wiegel T. Postoperative radiotherapy for advanced prostate cancer: improved local control translates into increased survival. Strahlenther Onkol 2009;185:485–487.
Schild SE, Buskirk SJ, Wong WW et al. The use of radiotherapy for patients with isolated elevation of serum prostate specific antigen following radical prostatectomy. J Urol 1996;156:1725–1729.
Shekarriz B, Upadhyay J, Wood DP, Jr. et al. Vesicourethral anastomosis biopsy after radical prostatectomy: predictive value of prostate-specific antigen and pathologic stage. Urology 1999;54:1044–1048.
Steil V, Schneider F, Kupper B et al. [Patient-centered image and data management in radiation oncology]. Strahlenther Onkol 2009;185:1–7.
Stephenson AJ, Scardino PT, Kattan MW et al. Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy. J Clin Oncol 2007;25:2035–2041.
Stephenson AJ, Shariat SF, Zelefsky MJ et al. Salvage radiotherapy for recurrent prostate cancer after radical prostatectomy. JAMA 2004;291:1325–1332.
Swindle P, Eastham JA, Ohori M et al. Do margins matter? The prognostic significance of positive surgical margins in radical prostatectomy specimens. J Urol 2008;179:S47–S51.
Thompson IM, Tangen CM, Paradelo J et al. Adjuvant radiotherapy for pathological T3N0M0 prostate cancer significantly reduces risk of metastases and improves survival: long-term follow-up of a randomized clinical trial. J Urol 2009;181:956–962.
Ward JF, Zincke H, Bergstralh EJ et al. Prostate specific antigen doubling time subsequent to radical prostatectomy as a prognosticator of outcome following salvage radiotherapy. J Urol 2004;172:2244–2248.
Wenz F, Martin T, Böhmer D et al. The German S3 guideline prostate cancer: aspects for the radiation oncologist. Strahlenther Oncol 2010;186:531–534.
Wiegel T, Bottke D, Steiner U et al. Phase III postoperative adjuvant radiotherapy after radical prostatectomy compared with radical prostatectomy alone in pT3 prostate cancer with postoperative undetectable prostate-specific antigen: ARO 96-02/AUO AP 09/95. J Clin Oncol 2009;27:2924–2930.
Wiegel T, Lohm G, Bottke D et al. Achieving an undetectable PSA after radiotherapy for biochemical progression after radical prostatectomy is an independent predictor of biochemical outcome-results of a retrospective study. Int J Radiat Oncol Biol Phys 2009;73:1009–1016.
Author information
Authors and Affiliations
Corresponding author
Additional information
*Both authors contributed equally to the manuscript
Rights and permissions
About this article
Cite this article
Siegmann, A., Bottke, D., Faehndrich, J. et al. Dose Escalation for Patients with Decreasing PSA during Radiotherapy for Elevated PSA after Radical Prostatectomy Improves Biochemical Progression-Free Survival. Strahlenther Onkol 187, 467–472 (2011). https://doi.org/10.1007/s00066-011-2229-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-011-2229-3