
Purpose:
To compare advanced treatment techniques with photons and protons as a stereotactic body radiation therapy (SBRT) for adrenal glands metastases.
Materials and Methods:
Planning computer tomographic (CT) scans of 10 patients were selected. A total dose of 45 Gy in 7.5 Gy fractions was prescribed. Organs at risk (OAR) were liver and kidneys. Dose–volume metrics were defined to quantify quality of plans assessing target coverage and sparing of organs at risk. Plans for RapidArc, intensity-modulated radiotherapy (IMRT), dynamic conformal arcs, 3D conformal static fields, and intensity modulated protons were compared. The main planning objective for the clinical target volume (CTV) was to cover 100% of the volume with 95% (V95% = 100%) and to keep the maximum dose below 107% of the prescribed dose (V107% = 0%). Planning objective for planning target volume (PTV) was V95% > 80%. For kidneys, the general planning objective was V15Gy < 35% and for liver V15Gy < (liver volume–700 cm3).
Results:
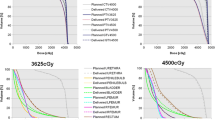
All techniques achieved the minimum and maximum dose objective for CTV and PTV, D5–95% ranged from 1 Gy (protons) to 1.6 Gy (conformal static fields) on CTV. Maximal organ at risk sparing was achieved by protons. RapidArc presented the second lowest dose bath (V10Gy and integral dose) after protons and the best conformality together with IMRT.
Conclusions:
Stereotactic body radiation therapy (SBRT) to adrenal glands metastases is achievable with several advanced techniques with either photons or protons. The intensity modulated approaches using either static fields, dynamic arcs or protons are superior to the other conformal solutions. For their simplicity, IMRT or RapidArc should be considered as the first option radiation treatment for those patients not eligible for proton treatment.
Ziel:
Diese Studie vergleicht fortgeschrittene Bestrahlungstechniken mit Photonen und Protonen bei der stereotaktischen Körperbestrahlung von Metastasen in Nebennieren.
Material und Methodik:
Es wurden Planungs-CTs von 10 Patienten ausgewählt und eine Dosis von 45 Gy mit einer Fraktionierungsdosis von 7.5 Gy verschrieben. Die Leber und die Nieren wurden als kritische Organe eingezeichnet. Es wurde eine Dosis-Volumen-Metrik zur Quantifizierung der Planqualität in Bezug auf die Zielvolumenabdeckung und die Schonung der kritischen Organe erstellt. RapidArc-, IMRT-, dynamisch konformale Rotations-, 3D konformale Pläne und intensitätsmodulierte Protonenpläne wurden verglichen. Die Planungsvorgaben für das CTV war die 100%ige Abdeckung des Volumens mit 95% der Verschreibungsdosis (V95% = 100%) und die Einhaltung einer maximalen Dosis unterhalb von 107% der Verschreibungsdosis (V107% = 0%). Die Planungsvorgabe für das PTV war V95% > 80%., für die Nieren V15Gy < 35% und für die Leber V15Gy < (Lebervolumen–700 cm3).
Ergebnisse:
Alle Bestrahlungstechniken erfüllten die minimalen und maximalen Dosisvorgaben für das CTV und das PTV.D5–95% reichten von 1 Gy (Protonen) bis zu 1,6 Gy (konformale statische Felder) beim CTV. Die maximale Schonung der kritischen Organe wurde mit der Protonentechnik erzielt. Die RapidArc-Technik zeigte das zweitniedrigste Dosisbad (V10Gy und integrale Dosis) nach den Protonen und die beste Konformität zusammen mit der IMRT-Technik.
Schlussfolgerung:
Die stereotaktische Körperbestrahlungstherapie von Metastasen in Nebennieren ist mit mehreren fortgeschrittenen Bestrahlungstechniken mit Photonen oder Protonen durchführbar. Die intensitätsmodulierten Methoden, entweder mit statischen Einstrahlrichtungen, dynamischen Rotationen oder Protonen, sind den anderen konformalen Techniken überlegen. Dank ihrer Einfachheit sollte die IMRT- oder die RapidArc-Technik als erste Option bei der Bestrahlung von Patienten, welche für eine Protonenbehandlung nicht in Frage kommen, berücksichtigt werden.
Similar content being viewed by others


References
Bignardi M, Cozzi L, Fogliata A et al. Critical appraisal of volumetric modulated arc therapy in stereotactic body radiation therapy for metastases to abdominal lymph nodes. Int J Radiat Oncol Biol Phys 2009;75:1570–7.
Bignardi M, Castiglioni S, Navarria P et al. Stereotactic body radiation therapy for metastases to abdominal lymph nodes. Radiother Oncol 2008;88(Supp 2):S235.
Chawla S, Chen Y, Katz A et al. Stereotactic body radiotherapy for treatment of adrenal metastases. Int J Radiat Oncol Biol Phys 2009;75:71–5.
Choi C, Cho C, Yoo S et al. Image-guided stereotactic body radiation therapy in patients with isolated para-aortic lymph node metastases from uterine cervical and corpus cancer. Int J Radiat Oncol Biol Phys 20089;74:147–53.
Cozzi L, Dinshaw KA, Shrivastava SK et al. A treatment planning study comparing volumetric arc modulation with RapidArc and fixed field IMRT for cervix uteri radiotherapy. Radiother Oncol 2008;89:180–91.
Cupp JS, Koong AC, Fisher GA et al. Tissue effects after stereotactic body radiotherapy using cyberknife for patients with abdominal malignancies. Clin Oncol 2008;20:69–75.
Dvorak P, Georg D, Bogner J et al. Impact of IMRT and leaf width on stereotactic body radiotherapy of liver and lung lesions. Int J Radiat Oncol Biol Phys 2005;61:1572–81.
Eccles CL, Bissonnette JP, Craig T et al. Treatment planning study to determine potential benefit of intensity-modulated radiotherapy versus conformal radiotherapy for unresectable hepatic malignancies. Int J Radiat Oncol Biol Phys 2008;72:582–8.
Eppinga W, Lagerwaard F, Verbakel W et al. Volumetric Modulated Arc Therapy for advanced pancreatic cancer. Strahlen Onkol 2010;186:382–7.
Fogliata A, Clivio A, Nicolini G et al. Intensity modulation with photons for benign intracranial tumours. A planning comparison of volumetric single arc, helical arc and fixed gantry techniques. Radiother Oncol 2008;89:254–62.
Fowler JF, Tomé WA, Fenwick JD et al. A challenge to traditional radiation oncology. Int J Radiat Oncol Biol Phys 2004;60:1241–56.
Hoyer M, Roed H, Traberg Hansen A et al. Phase II study on stereotactic body radiotherapy of colorectal metastases. Acta Oncol 2006;45:823–30.
Jacob V, Bayer W, Astner S et al. A planning comparison of dynamic IMRT for different collimator leaf thicknesses with helical tomotherapy and Rapidarc for prostate and head and neck tumors. Strahlenther Onkol 2010;186:502–10.
Katoh N, Onimaru R. Sakuhara Y et al. Real time tumor-tracking radiotherapy for adrenal tumors Radiother Oncol 87;2008:418–24.
Kim S, Brennan M, Russo P, et al. The role of surgery in the treatment of clinically isolated adrenal metastasis. Cancer 1998;82:389–94.
Lam K, Lo C. Metastatic tumors of the adrenal glands. A 30 year experience in a teaching hospital. Clin Endocrinol 2002;56:95–101.
Lomax A, Pedroni E, Schaffner B et al. A 3D treatment planning for conformal proton therapy by spot scanning. In: Faulkner K, Carey B, Crellin A, Harrison RM (eds) Quantitative imaging in oncology. BIR publishing, London 1996, pp 67–71.
Macdermed DM, Weichselbaum RR, Salama JK. A rationale for the targeted treatment of oligometastases with radiotherapy. J Surg Onco. 2008;98:202–6.
Milano MT, Katz AW, Schell MC et al. Descriptive analysis of oligometastatic lesions treated with curative-intent stereotactic body radiotherapy. Int J Radiat Oncol Biol Phys 2008;72:1516–22.
Miyaji N, Miki T, Itoh Y et al. Radiotherapy for adrenal gland metastasis from lung cancer. Report of three cases. Radiat Med 1999;17:71–5.
Nuyttens JJ, Prevost JB, Van der Voort van Zijp NC et al. Curative stereotactic robotic radiotherapy treatment for extracranial, extrapulmonary, extrahepatic, and extraspinal tumors: technique, early results, and toxicity. Technol Cancer Res Treat 2007;6:605–.10.
Otto K. Volumetric modulated arc therapy: IMRT in a single arc. Med Phys 2008;35:310–7.
Short S, Chaturvedi A, Leslie M. Palliation of symptomatic adrenal gland metastases by radiotherapy. Clin Oncol 1996;8:387–9.
Soffen E, Solin L, Rubenstein J. Palliative radiotherapy for symptomatic adrenal metastases. Cancer 1990;65:1318–20.
Teh BS, Paulino AC, Lu HH et al. Versatility of the Novalis system to deliver image-guided stereotactic body radiation therapy (SBRT) for various anatomical sites. Technol Cancer Res Treat 2007;6:347–54.
Timmerman RD, Kavanagh BD, Cho LC et al. Stereotactic body radiation therapy in multiple organ sites. J Clin Oncol 2007;25:947–52.
Ulmer W. Theoretical aspects of energy range relations, stopping power and energy straggling of protons. Radiat Phys and Chem 2007;76:1089–107.
Vandecasteele K, De Neve W, De Gersem W et al. Intensity modulated arc therapy with simultaneous integrated boost in the treatment of primary irresectable cervical cancer. Treatment planning, quality control and clinical implementation. Strahlenther Onkol 2009;185:799–807.
Vanetti E, Clivio A, Nicolini G et al. Volumetric modulated arc radiotherapy for carcinomas of the oro-pharynx, hypo-pharynx and larynx: a treatment planning comparison with fixed field IMRT. Radiother Oncol 2009; 92:111–7.
Verbakel WF, Senan S, Cuijpers JP et al. Rapid delivery of stereotactic radiotherapy for peripheral lung tumors using volumetric intensity-modulated arcs. Radiother Oncol 2009;93:122–4.
Wood B, Abraham J, Hvizda J et al. Radiofrequency ablation of adrenal tumors and adrenocortical carcinoma metastases. Cancer 2003;97:554–60.
Wolf D, Stieler F, Hermann B et al. Clinical implementation of volumetric intensity modulated arc therapy (VMAT) with ERGO++. Strahlenther Onkol 2010;186:280–8.
Zeng Z, Tang Z, Fan J. Radiation therapy for adrenal gland metastases from hepatocellular carcinoma. Jpn J Clin Oncol 2005;35:61–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Scorsetti, M., Mancosu, P., Navarria, P. et al. Stereotactic Body Radiation Therapy (SBRT) for adrenal metastases. Strahlenther Onkol 187, 238–244 (2011). https://doi.org/10.1007/s00066-011-2207-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-011-2207-9