
Purpose:
To retrospectively assess the incidence and time course of renal dysfunction in children (≤ 16 years) following total- body irradiation (TBI) before allogeneic stem cell transplantation (SCT).
Patients and Methods:
Between 1986 and 2003, 92 children (median age, 11 years; range, 3–16 years) underwent TBI before allogeneic SCT. 43 of them had a minimum follow-up of 12 months (median, 51 months; range, 12–186 months) and were included into this analysis. Conditioning regimen included chemotherapy and fractionated TBI with 12 Gy (n = 26) or 11.1 Gy (n = 17). In one patient, renal dose was limited to 10 Gy by customized renal shielding due to known nephropathy prior to SCT. Renal dysfunction was defined as an increase of serum creatinine > 1.25 times the upper limit of age-dependent normal.
Results:
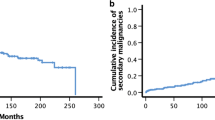
Twelve children (28%) experienced an episode of renal dysfunction after a median of 2 months (range, 1–10 months) following SCT. In all but one patient renal dysfunction was transient and resolved after a median of 8 months (range, 3–16 months). One single patient developed persistent renal dysfunction with onset at 10 months after SCT. None of these patients required dialysis. The actuarial 3-year freedom from persistent renal toxicity for children surviving > 12 months after SCT was 97.3%.
Conclusion:
The incidence of persistent renal dysfunction after fractionated TBI with total doses ≤ 12 Gy was very low in this analysis.
Ziel:
In einer retrospektiven Analyse wurden die Inzidenz und der zeitliche Verlauf der renalen Spattoxizitat bei Kindern (≤ 16 Jahre) nach Ganzkorperbestrahlung (TBI) vor allogener Stammzelltransplantation (SCT) untersucht.
Patienten und Methodik:
Von 1986 bis 2003 erhielten 92 Kinder (medianes Alter 11 Jahre; Streubreite 3–16 Jahre) eine fraktionierte TBI vor allogener SCT. 43 Patienten wiesen eine Nachbeobachtungszeit von mindestens 12 Monaten auf (median 51 Monate; Streubreite 12–186 Monate) und gingen in diese Analyse ein. Die Konditionierung bestand aus einer Chemotherapie und einer fraktionierten TBI mit 12 Gy (n = 26) bzw. 11,1 Gy (n = 17). Bei einem Patienten wurde aufgrund einer vorbestehenden Nephropathie die Nierendosis durch individuelle Ausblockung auf 10 Gy begrenzt. Als renale Dysfunktion wurde ein Anstieg des Serumkreatinins uber das 1,25fache des jeweils altersabhangigen oberen Grenzwerts nach SCT definiert.
Ergebnisse:
Zwolf Kinder (28%) entwickelten eine renale Dysfunktion median 2 Monate nach SCT (Streubreite 1–10 Monate). Bei elf dieser Patienten war die renale Dysfunktion temporar mit Normalisierung nach median 8 Monaten (Streubreite 3–16 Monate). Nur bei einem Kind lag eine persistierende renale Dysfunktion vor, die 10 Monate nach SCT auftrat. Keines dieser Kinder wurde dialysepflichtig. Die aktuarische 3-Jahres-Freiheit von persistierenden renalen Funktionseinschrankungen bei Kindern mit einem Nachbeobachtungszeitraum von mindestens 12 Monaten nach SCT betrug 97,3%.
Schlussfolgerung:
Die Inzidenz einer persistierenden renalen Dysfunktion nach fraktionierter TBI mit einer Gesamtdosis ≤ 12 Gy war in dieser Analyse sehr niedrig.
Similar content being viewed by others

References
Belka C, Budach W, Betsch A, et al. Ganzkörperbestrahlung für die Knochenmark-/Blutstammzelltransplantation. Onkologe 2001;7:1305–1312.
Belkacémi Y, Pene F, Touboul E, et al. Total-body irradiation prior to bone marrow transplantation for acute leukemia. Strahlenther Onkol 1998;174:92–104.
Bölling T, Könnemann S, Willich N. Late effects of thoracic irradiation in children. Strahlenther Onkol 2008;184:289–295.
Bölling T, Schuck A, Rübe C, et al. Behandlungsassoziierte Spätfolgen nach Strahlentherapie maligner Erkrankungen im Kindes- und Jugendalter. Strahlenther Onkol 2006;182:443–449.
Borg M, Hughes T, Horvath N, et al. Renal toxicity after total body irradiation. Int J Radiat Oncol Biol Phys 2002;54:1165–1173.
Cheng JC, Schultheiss TE, Wong JYC. Impact of drug therapy, radiation dose and dose rate on renal toxicity following bone marrow transplantation. Int J Radiat Oncol Biol Phys 2008;71:1436–1443.
Chou RH, Wong GB, Kramer JH, et al. Toxicities of total-body irradiation for pediatric bone marrow transplantation. Int J Radiat Oncol Biol Phys 1996;34:843–851.
Cohen EP. Renal failure after bone marrow transplantation. Lancet 2001;357:6–7.
Deconinck E, Cahn JY. Renal toxicity after bone marrow transplantation. Int J Radiat Oncol Biol Phys 2004;58:661–662.
Dörr W, Herrmann T. Second tumors after oncologic treatment. Strahlenther Onkol 2008;184:67–72.
Esiashvili N, Chiang KY, Hasselle MD, et al. Renal toxicity in children undergoing total body irradiation for bone marrow transplant. Radiother Oncol 2009;90:242–246.
Fajardo LF, Brown JM, Glatstein E. Glomerular and juxta-glomerular lesions in radiation nephropathy. Radiat Res 1976;68:177–183.
Frisk P, Bratteby LE, Carlson K, et al. Renal function after autologous bone marrow transplantation in children: a long-term prospective study. Bone Marrow Transplant 2002;29:129–136.
Grönroos MH, Bolme P, Winiarski J, et al. Long-term renal function following bone marrow transplantation. Bone Marrow Transplant 2007;39:717–723.
Heinzelmann F, Ottinger H, Müller CH, et al. Total body irradiation — role and indications. Results from the German Registry from Stem Cell Transplantation (DRST). Strahlenther Onkol 2006;182:222–230.
Igaki H, Karasawa K, Sakamaki H, et al. Renal dysfunction after total-body irradiation. Strahlenther Onkol 2005;181:704–708.
Kal HB, van Kempen-Harteveld ML. Renal dysfunction after total body irradiation: dose-effect relationship. Int J Radiat Oncol Biol Phys 2006;65:1228–1232.
Kal HB, van Kempen-Harteveld ML, Heijenbrok-Kal MH, et al. Biologically effective dose in total-body irradiation and hematopoietic stem cell transplantation. Strahlenther Onkol 2006;182:672–679.
Kist-van Holthe JE, Goedvolk CA, Brand R, et al. Prospective study of renal insufficiency after bone marrow transplantation. Pediatr Nephrol 2002;17:1032–1037.
Lawton CA, Cohen EP, Murray KJ, et al. Long-term results of selective renal shielding in patients undergoing total body irradiation in preparation for bone marrow transplantation. Bone Marrow Transplant 1997;20:1069–1074.
Miralbell R, Bieri S, Mermillod B, et al. Renal toxicity after allogeneic bone marrow transplantation: the combined effects of total-body irradiation and graft-versus-host-disease. J Clin Oncol 1996;14:579–585.
Miralbell R, Sancho G, Bieri S, et al. Renal insufficiency in patients with hematologic malignancies undergoing total body irradiation and bone marrow transplantation: a prospective assessment. Int J Radiat Oncol Biol Phys 2004;58:809–816.
Nevinny-Stickel M, Poljanc K, Forthuber BC, et al. Optimized conformal paraaortic lymph node irradiation is not associated with enhanced renal toxicity. Strahlenther Onkol 2007;183:385–391.
Ramm U, Licher J, Moog J, et al. In vivo dosimetry with semiconducting diodes for dose verification in total body irradiation. Strahlenther Onkol 2008;184:376–380.
Röttinger EW, Bartkowiak D, Bunjes D, et al. Enhanced renal toxicity of total body irradiation combined with radioimmuntherapy. Strahlenther Onkol 2003;179:702–707.
Schneider RA, Schultze J, Jensen JM, et al. 20 years of experience in static intensity-modulated total-body irradiation and lung toxicity. Strahlenther Onkol 2007;183:545–551.
Strenger V, Sovinz P, Lackner H, et al. Intracerebral cavernous hemangioma after cranial irradiation in childhood. Strahlenther Onkol 2008;184:276–280.
Wheldon TE, Barret A. Radiobiological modelling of the treatment of leukaemia by total body irradiation. Radiother Oncol 2001;58:227–233.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gerstein, J., Meyer, A., Sykora, KW. et al. Long-Term Renal Toxicity in Children Following Fractionated Total-Body Irradiation (TBI) Before Allogeneic Stem Cell Transplantation (SCT). Strahlenther Onkol 185, 751–755 (2009). https://doi.org/10.1007/s00066-009-2022-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-009-2022-8