
Abstract
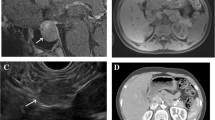
We report the case of a patient presenting amenorrhea, hyperprolactinemia, headache and nuclear magnetic resonance (NMR) evidence of pituitary macroadenoma. The family history revealed that the patient’s father had had a referred sporadic insulinoma, removed 25 yr before without evidence of other endocrine disorders. Physical examination evidenced a slight neck enlargement. Among biochemical and endocrinological assays performed, only hyperprolactinemia was observed. Neck ultrasonography (US) revealed a parathyroid enlargement and a 99mTcO4/MIBI scan showed two hyperplasic lesions. Considering the diagnostic suspect of multiple endocrine neoplasia (MEN1), we performed abdominal US and NMR studies, showing a pancreatic lesion compatible with neuroendocrine tumor. A total body 111In-DTPA-d-Phe1-octreotide scan (Octreoscan®) was also carried out, evidencing no pituitary tumor uptake but high uptake of the abdominal lesion. After surgery, the histological examination confirmed the two parathyroid adenomas and four non-functioning pancreatic neuroendocrine tumors. When the patient was admitted for studying the pituitary lesion and for planning the opportune therapy, an early and partially subclinical stage of MEN1 was identified, potentially already clear but otherwise undiagnosed, and the genetic state of the patient’s relatives, as possible carriers of DNA mutation, was checked. The DNA study for germline mutations confirmed the clinical diagnosis of MEN1 syndrome in the patient and evidenced the same MEN1 mutation in her father and twin sister. In this case report, we would like to underline that, still today, a correct anamnesis and physical examination are the cornerstone of clinical approach to the patient. Furthermore, initial good practice approach is necessary to plan the diagnostic iter, enabling clinicians to decide upon the best orientation and interpretation of the results among several complicated and expensive exams.
Similar content being viewed by others


References
Arafah BM, Nasrallah MP. Pituitary tumors: pathophysiology, clinical manifestations and management. Endocr Related Cancer 2001, 8: 287–305.
Lubke D, Saeger W. Carcinomas of the pituitary: definition and review of the literature. Gen diagn path 1995, 141: 81–92.
Corbetta S, Pizzocaro A, Peracchi M, Beck-Peccoz P, Faglia G, Spada A. Multiple endocrine neoplasia type 1 in patients with recognized pituitary tumours of different types. Clin Endocrinol (Oxf) 1997, 47: 507–12.
Brandi ML, Gagel RF, Angeli A, et al. Guidelines for diagnosis and therapy of MEN type 1 and type 2. J Clin Endocrinol Metab 2001, 86: 5658–71.
Thakker RV. Multipe endocrine neoplasia. Horm Res 2001, 56 (Suppl 1): 67–72.
Kaczirek K, Prager G, Schindl M, et al. Multiple endocrine neoplasia 1 — Current recommendations for diagnosis and treatment. Wien Klin Wochenschr 2002, 114: 258–66.
Marsh D, Zori R. Genetic insights into familial cancers — update and recent discoveries. Cancer Lett 2002, 181: 125–64.
Carty SE, Helm AK, Amico JA, et al. The variable penetrance and spectrum of manifestations of multiple endocrine neoplasia type 1. Surgery 1998, 124: 1106–14.
Verges B, Boureille F, Goudet P, et al. Pituitary disease in MEN type 1 (MEN1): data from the France-Belgium MEN1 multicenter study. J Clin Endocrinol Metab 2002, 87: 457–65.
Giordano A, Rubello D, Casara D. New trends in parathyroid scintigraphy. Eur J Nucl Med 2001, 28: 1409–20.
Zarnegar R, Brunaud L, Clark OH. Multiple endocrine neoplasia type I. Curr Treat Options Oncol 2002, 3: 35–48.
Perez-Monte JE, Brown ML, Clarke MR, Watson CG, Carty SE. Parathyroid hyperplasia, thymic carcinoid and pituitary adenoma detected with technetium-99mMIBI in MEN type I. J Nucl Med 1997, 38: 1767–9.
Nguyen BD, Wang EA. Multiple endocrine neoplasia type 1: scintigraphic and magnetic resonance demonstration. Clin Nucl Med 1999, 24: 73–4.
Fidler JL, Johnson CD. Imaging of neuroendocrine tumors of the pancreas. Int J Gastrointest Cancer 2001, 30: 73–85.
van Eijck CH, Lamberts SW, Lemaire LC, et al. The use of somatostatin receptor scintigraphy in the differential diagnosis of pancreatic duct cancers and islet cell tumors. Ann Surg 1996, 224: 119–24.
Krausz Y, Bar-Ziv J, de Jong RBJ, et al. Somatostatin-receptor scintigraphy in the management of gastroenteropancreatic tumors. Am J Gastroenterol 1998, 93: 66–70.
Skogseid B, Öberg K, Äkerström G, et al. Limited tumor involvement found at multiple endocrine neoplasia type 1 pancreatic exploration: can it be predicted by preoperative tumor localization? World J Surg 1998, 22: 673–8.
Shimon I, Yan X, Taylor JE, Weiss MH, Culler MD, Melmed S. Somatostatin receptor (SSTR) subtype-selective analogues differentially suppress in vitro growth hormone and prolactin in human pituitary adenomas. Novel potential therapy for functional pituitary tumors. J Clin Invest 1997, 100: 2386–92.
Jacquet P, Ouafik L, Saveanu A, et al. Quantitative and functional expression of somatostatin receptor subtypes in human prolactinomas. J Clin Endocrinol Metab 1999, 84: 3268–76.
Lamberts SWJ, van der Lely AJ, Hofland LJ. New somatostatin analogs: will they fulfil old promises. Eur J Endocrinol 2002, 146: 701–5.
Zatelli MD, Piccin D, Franceschetti P, et al. Dopamine-resistant invasive macroprolactinoma: from bench to bedside. J Endocrinol Invest 2002, 25 (Suppl 6): 18 (abstract).
Lamberts SWJ, Verleun T, Hofland L, Del Pozo E. A comparison between the effects of SMS201-995, bromocriptine and the combination of both drugs on hormone release by cultured pituitary tumor cells of acromegalic patients. Clin Endocrinol (Oxf) 1987, 27: 11–23.
Wagenaar AH, Harris AG, Van der Lely AJ, Lamberts SWJ. Dynamic of the acute effects of octreotide, bromocriptine and both drugs in combination on growth hormone secretion in acromegaly. Acta Endocrinol (Copenh) 1991, 125: 637–42.
Fredstorp L, Kutz K, Werner S. Treatment with octreotide and bromocriptine in patients with acromegaly: an open phamacodynamic interaction study. Clin Endocrinol (Oxf) 1994: 41: 103–8.
Flogstad AK, Halse J, Grass P, et al. A comparison of octreotide, bromocriptine, or a combination of both drugs in acromegaly. J Clin Endocrinol Metab 1994, 79: 461–5.
Abs R, Verhelst J, Master D, et al. Cabergoline in the treatment of acromegaly: a study in 64 patients. J Clin Endocrinol Metab 1998, 83: 374–8.
Barzon L, Pasquali C, Grigoletto C, Pedrazzoli S, Boscaro M, Fallo F. Multiple Endocrine Neoplasia type 1 and adrenal lesions. J Urol 2001, 166: 24–7.
Ringe D. Function by serendipity. Nature 2002, 415: 488–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tamagno, G., De Carlo, E., Martini, C. et al. The early diagnosis of multiple endocrine neoplasia type 1 (MEN 1): A case report. J Endocrinol Invest 27, 878–882 (2004). https://doi.org/10.1007/BF03346285
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03346285