
Abstract
Purpose
To assess the survival rate, the probability of local control, the patterns of relapse and late sequelae including self-reported quality of life in patients treated with hyperfractionated radiotherapy (RT) and simultaneous CDDP chemotherapy for stage-III to stage-IV carcinomas of the head and neck.
Methods
From 1988 to 1994, 64 patients (median age 55.5 years) with carcinomas of different subsites, excluding the nasopharynx, were treated in a pilot study with 1.2 Gy bid (6 h interval; total dose 74.4 Gy) and simultaneous CDDP (20 mg/m2 daily, 5 days in week 1 and 5) and followed at regular intervals. Overall survival and local control, as well as the rates of late toxicity, were estimated using the actuarial method. Median follow-up was 3.3 years for all and 5.2 years for surviving patients. To assess the quality of life, the EORTC QLQ-C 30 questionnaire and the H&N35 module questionnaire were sent to the patients surviving with no evidence of disease or second primary tumors; they were answered by 15/23 (67%).
Results
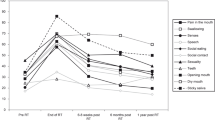
Overall survival was 37% at 5 years, whereas disease-specific survival was 59%. Twenty-three patients died from uncontrolled head and neck cancer. Second primary tumors were observed in 13 patients, most frequently in the lung. Local control without salvage surgery was 74% at 5 years for all subsites and stages, and loco-regional disease-free survival was 72%. Eleven patients developed distant metastases, which was the only site of failure in 6 cases. Salvage surgery was successful in 2 cases. The actuarial estimates of ≥ grade-3 late toxicity was 4% for the mandibular bone and 23% for dysphagia, and 50% of the patients experienced a permanent xerostomy. Self-reported global quality of life in surviving patients was good (mean 68 points on a scale 0 to 100); consequences of impaired salivary function had most impact on nutritional and social aspects.
Conclusions
Hyperfractionated RT with concomitant CDDP is well tolerated and highly efficient in controlling moderately advanced to advanced cancers of the head and neck. Second primary tumors are the main cause of death after 3 years and were observed outside of the irradiated area, most frequently in the lung. Even after RT of large volumes to a high dose, salvage surgery can be successfully performed in individual cases. Self-reported quality of life of surviving patients is good, despite xerostomy-associated nutritional difficulties.
Zusammenfassung
Ziel
Analyse der Überlebensrate, des krankheitsspezifischen Überlebens, des Rezidivmusters, der Spättoxizität sowie der subjektiven Lebensqualität nach hyperfraktionierter Radiotherapie (RT) und gleichzeitiger Cisplatin-Chemotherapie (CDDP) bei Patienten mit mindestens zwei Jahren Beobachtungszeit im Rahmen einer prospektiven Phase-II-Studie.
Patienten und Methode
Im Rahmen einer Pilotstudie (1988 bis 1994) wurden 64 Patienten (medianes Alter 55,5 Jahre) mit Stadium III oder IV kombiniert behandelt: RT 1,2 Gy zweimal täglich bis 74,4 Gy, CDDP 20 mg/m2 täglich an den Tagen 1 bis 5 der ersten und fünften Woche. Die Überlebenskurven sowie die Toxizität wurden aktuariell berechnet. Die mediane Beobachtungszeit war 3,3 Jahre für alle respektive 5,2 Jahre für die überlebenden Patienten. Zur Einschätzung der Lebensqualität wurden 23 tumorfrei überlebende Patienten angefragt, den EORTC-QLQ-C30-Fragebogen sowie das ergänzende Modul für Kopf-Hals-Tumoren H&N35 auszufüllen.
Ergebnisse
Das Gesamtüberleben betrug nach fünf Jahren 37%, während das krankheitsspezifische Überleben mit 59% deutlich höher lag. 23 Patienten sind am Tumor verstorben. Zweittumoren, hauptsächlich Lungenkarzinome (n=8), wurden bei 13 Patienten registriert und waren die hauptsächliche Todesursache nach über drei Jahren. Die lokale Tumorkontrolle ohne zusätzliche Chirurgie betrug 74% nach fünf Jahren und war für alle Lokalisationen und Stadien gleich; die lokoregionäre Tumorkontrollrate lag bei 64%. Fernmetastasen ohne ein lokoregionäres Therapieversagen wurden bei sechs Patienten gesehen. Eine „Rettungschirurgie” wurde in zwei Fällen erfolgreich durchgeführt. Die aktuarielle Spätkomplikationsrate ≥ Grad 3 betrug 4% für den Kieferknochen und 23% für Dysphagie; 50% der Patienten hatten eine bleibende komplette Xerostomie. Die globale Lebensqualität war gut (im Mittel 68 Punkte auf einer Skala von 0 bis 100). Folgen der gestörten Speichelsekretion hatten die größte Auswirkung auf die funktionelle Behinderung der Ernährung sowie der sozialen Kontakte.
Schlußfolgerungen
Die hyperfraktionierte RT mit gleichzeitiger CDDP-Gabe wird hinsichtlich Spättoxizität gut toleriert und ist effizient zur Behandlung fortgeschrittener Kopf-Hals-Tumoren. Im Gegensatz zu chirurgischen Serien treten Zweitkarzinome praktisch nur außerhalb des ursprünglichen Tumorbereichs auf. Eine „Rettungschirurgie” nach initialem Therapieversagen ist auch nach RT mit 74,4 Gy in Einzelfällen erfolgreich. Die selbstrapportierte Lebensqualität bei den Langzeitüberlebenden ist generell gut trotz gewisser, vorwiegend xerostomiebedingter Einschränkungen.
Similar content being viewed by others


References
Aaronson NK, Ahmedzai S, Bergman B, et al. QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993;85:365–76.
Bjordal K, Ahlner-Elmqvist M, Tollesson E, et al. Development of a European Organization for Research and Treatment of Cancer (EORTC) questionnaire module to be used in quality-of-life assessments in head and neck cancer patients. Acta Oncol 1994;33:879–85.
Bjordal K, Freng A, Thorvik J, et al. Patient self-reported and clinicianrated quality of life in head and neck cancer patients: a cross-sectional study. Eur J Cancer 1995;31B:235–41.
Choi KN, Rotman M, Aziz H, et al. Locally advanced paranasal sinus and nasopharynx tumors treated with hyperfractionated radiation and concomitant infusion of cisplatin. Cancer 1991;67:2748–52.
Cooper KN, Rotman M, Aziz H, et al. Second malignancies in patients who have head and neck cancer: incidence, effect on survival and implications based on the RTOG experience. Int J Radiat Oncol Biol Phys 1989;17:449–56.
Dühmke E, Geibel T, Golms G, et al. Combined modality treatment of advanced head and neck cancer using low-dose cisplatinum and accelerated fractionation. Strahlenther Onkol 1988;164:11–6.
Glanzmann C, Lütolf UM. Follow-up data of our pilot study on concomitant hyperfractionated radiotherapy and cisplatinum (CDDP) in patients with advanced cancer of the head and neck. Strahlenther Onkol 1992;168:453–6.
Harrison LB, Pfister DG, Fass DE, et al. Concomitant chemotherapy and radiation therapy for advanced unresectable head and neck cancer. Int J Radiat Oncol Biol Phys 1991;21:703–8.
Hong WK, Lippman SM, Itri LM, et al. Prevention of second primary tumors with isotrtinoin in squamous-cell carcinoma of the head and neck. N Engl J Med 1990;323:795–801.
Horiot JC, Le Fur R, N’Guyen TN, et al. Hyperfractionation versus conventional fractionation in oropharyngeal carcinoma: final analysis of a randomized trial of the EORTC cooperative group of radiotherapy. Radiother Oncol 1992;25:231–41.
Marcial VA, Pajak TF, Mohuddin M, et al. Concomitant cisplatin chemotherapy and radiotherapy in advanced mucosal squamous-cell carcinomas of the head and neck. Cancer 1990;66:1861–8.
Mendenhall WM, Parsons JT. Letter to the editor. N Engl J Med 1993;328:579–80.
Merlano M, Benasso M, Corvò R, et al. Five-year update of a randomized trial of alternating radiotherapy and chemotherapy compared with radiotherapy alone in treatment of unresectable squamous-cell carcinoma of the head and neck. J Natl Cancer Inst 1996;88:583–9.
Merlano M, Vitale V, Rosso R, et al. Treatment of advanced squamouscell carcinoma of the head and neck with alternating chemotherapy and radiotherapy. N Engl J Med 1992;327:1115–21.
Munro AJ. An overview of randomized controlled trials of adjuvant chemotherapy in head and neck cancer. Br J Cancer 1995;71:83–91.
Parsons JT. Time-dose-volume relations in radiation therapy. In Million RR, Cassisi NJ (Eds) Management of head and neck cancer, Philadelphia: Lippincott, 1994:203–43.
Pinto LHJ, Canary PCV, Araucho CMM, et al. Prospective randomized trial comparing hyperfractionated versus conventional radiotherapy in stages III and IV oropharyngeal carcinoma. Int J Radiat Oncol Biol Phys 1991;21:557–62.
Seegenschmiedt MH, Sauer R. Systematik der akuten und chronischen Strahlenfolgen. Strahlenther Onkol 1993;169:83–95.
Stell PM, Rawson NSB. Adjuvant chemotherapy in head and neck cancer. Br J Cancer 1990;61:779–87.
Vokes E E, Weichselbaum RR. Concomitant chemoradiotherapy: rationale and clinical experience in patients with solid tumors. J Clin Oncol 1990;8:911–34.
Vokes EE, Weichselbaum RR. Radiotherapy with concomitant chemotherapy for head and neck cancer. Haematol Oncol Clin North Am 1991;5:753–67.
Wendt TG. Radiochemotherapie bei fortgeschrittenen Kopf-Hals-Tumoren — was ist gesichert? Strahlenther Onkol 1996;172:409–16.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Huguenin, P., Glanzmann, C., Taussky, D. et al. Hyperfractionated radiotherapy and simultaneous cisplatin for stage-III and-IV carcinomas of the head and neck. Strahlenther Onkol 174, 397–402 (1998). https://doi.org/10.1007/BF03038560
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03038560