
Abstract
Purpose
The purpose of this study is to determine if real time ultrasound guidance improves the success rate of axillary brachial plexus blockade.
Methods
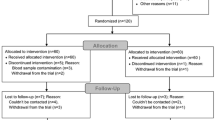
Patients undergoing elective hand surgery were randomly assigned to one of three groups. Axillary blocks were performed using three motor response endpoints in the nerve stimulator (NS) Group, real-time ultrasound guidance in the ultrasound (US) Group and combined ultrasound and nerve stimulation in the USNS Group. Following administration of a standardized solution containing 2% lidocaine with 1:200,000 epinephrine and 0.5% bupivacaine (total 42 mL), sensory and motor functions were assessed by a blinded observer every five minutes for 30 min. A successful block was defined as complete sensory loss in the median, radial and ulnar nerve distribution by 30 min. The need for local and general anesthesia supplementation and post-block adverse events were documented.
Results
One hundred and eighty-eight patients completed the study. Block success rate was higher in Groups US and USNS (82.8% and 80.7%) than Group NS (62.9%) (P = 0.01 and 0.03 respectively). Fewer patients in Groups US and USNS required supplemental nerve blocks and/or general anesthesia. Postoperatively, axillary bruising and pain were reported more frequently in Group NS.
Conclusion
This study demonstrates that ultrasound guidance, with or without concomitant nerve stimulation, significantly improves the success rate of axillary brachial plexus block.
Résumé
Objectif
Le but de cette étude est de déterminer si l’échoguidage en temps réel améliore le taux de succès du bloc du plexus brachial par approche axillaire.
Méthode
Des patients devant subir une chirurgie élective de la main ont été randomisés en trois groupes. Des blocs axillaires ont été effectués en utilisant: trois points de réponses motrices dans le groupe neurostimulateur (NS), l’échoguidage en temps réel dans le groupe échographie (EG), et l’échographie combinée à la stimulation nerveuse dans le troisième groupe (EGNS). Suite à l’administration d’une solution standardisée contenant de la lidocaïne 2 % avec épinéphrine (1:200 000) et de la bupivacaïne 0,5 % (total 42 mL), les fonctions sensitives et motrices ont été évaluées par un observateur neutre toutes les cinq minutes pendant 30 min. Un bloc réussi a été défini comme la perte complète de sensation dans la distribution des nerfs médian, radial et cubital après 30 min. La nécessité d’une anesthésie locale et générale supplémentaire ainsi que les effets négatifs post-bloc ont été documentés.
Résultat
Chez les 188 patients qui ont terminé l’étude, le taux de succès du bloc a été plus élevé dans les groupes EG et EGNS (82,8 % et 80,7 %) que dans le groupe NS (62,9 %) (P) =0,01 et 0,03 respectivement). Un nombre moins élevé de patients des groupes EG et EGNS a nécessité des blocs nerveux supplémentaires et/ou une anesthésie générale. Après l’opération, les hématomes et douleurs axillaires ont été plus fréquemment observés dans le groupe NS.
Conclusion
Cette étude démontre que l’échoguidage, avec ou sans neurostimulation concomitante, améliore de façon significative le taux de succès du bloc du plexus brachial par approche axillaire.
Article PDF
Similar content being viewed by others


References
Pavlin DJ, Rapp SE, Polissar NL, Malmgren JA, Koerschgen M, Keyes H. Factors affecting discharge time in adult outpatients. Anesth Analg 1998; 87: 816–26.
Chan VW, Peng PW, Kaszas Z, et al. A comparative study of general anesthesia, intravenous regional anesthesia, and axillary block for outpatient hand surgery: clinical outcome and cost analysis. Anesth Analg 2001; 93: 1181–4.
Ben David B, Stahl S. Axillary block complicated by hematoma and radial nerve injury. Reg Anesth Pain Med 1999; 24: 264–6.
Stark RH. Neurologic injury from axillary block anesthesia. J Hand Surg (Am) 1996; 21: 391–6.
Stan TC, Krantz MA, Solomon DL, Poulos JG, Chaouki K. The incidence of neurovascular complications following axillary brachial plexus block using a transarterial approach. A prospective study of 1,000 consecutive patients. Reg Anesth 1995; 20: 486–92.
Perlas A, Chan VW, Simons M. Brachial plexus examination and localization using ultrasound and electrical stimulation: a volunteer study. Anesthesiology 2003; 99: 429–35.
De Andres J, Sala-Blanch X. Ultrasound in the practice of brachial plexus anesthesia. Reg Anesth Pain Med 2002; 27: 77–89.
Chan VW. Applying ultrasound imaging to interscalene brachial plexus block. Reg Anesth Pain Med 2003; 28: 340–3.
Chan VW, Perlas A, Rawson R, Odukoya O. Ultrasound-guided supraclavicular brachial plexus block. Anesth Analg 2003; 97: 1514–7.
Ootaki C, Hayashi H, Amano M. Ultrasound-guided infraclavicular brachial plexus block: an alternative technique to anatomical landmark-guided approaches. Reg Anesth Pain Med 2000; 25: 600–4.
Sandhu NS, Capan LM. Ultrasound-guided infraclavicular brachial plexus block. Br J Anaesth 2002; 89: 254–9.
Ting PL, Sivagnanaratnam V. Ultrasonographic study of the spread of local anaesthetic during axillary brachial plexus block. Br J Anaesth 1989; 63: 326–9.
Reed J, Leighton S. Ultrasound facilitation of brachial plexus block. Anaesth Intensive Care 1994; 22: 499.
Retzl G, Kapral S, Greher M, Mauritz W. Ultrasonographic findings of the axillary part of the brachial plexus. Anesth Analg 2001; 92: 1271–5.
Schwemmer U, Markus CK, Greim CA, Brederlau J, Roewer N. Ultrasound-guided anaesthesia of the axillary brachial plexus: efficacy of multiple injection approach. Ultraschall Med 2005; 26: 114–9.
Williams SR, Chouinard P, Arcand G, et al. Ultrasound guidance speeds execution and improves the quality of supraclavicular block. Anesth Analg 2003; 97: 1518–23.
Liu FC, Liou JT, Tsai YF, et al. Efficacy of ultrasound- guided axillary brachial plexus block: a comparative study with nerve stimulator-guided method. Chang Gung Med J 2005; 28: 396–402.
Marhofer P, Sitzwohl C, Greher M, Kapral S. Ultrasound guidance for infraclavicular brachial plexus anaesthesia in children. Anaesthesia 2004; 59: 642–6.
Soeding PE, Sha S, Royse CE, Marks P, Hoy G, Royse AG. A randomized trial of ultrasound-guided brachial plexus anaesthesia in upper limb surgery. Anaesth Intensive Care 2005; 33: 719–25.
Sites BD, Beach ML, Spence BC, et al. Ultrasound guidance improves the success rate of a perivascular axillary plexus block. Acta Anaesthesiol Scand 2006; 50: 678–84.
Sia S, Bartoli M, Lepri A, Marchini O, Ponsecchi P. Multiple-injection axillary brachial plexus block: a comparison of two methods of nerve localization-nerve stimulation versus paresthesia. Anesth Analg 2000; 91: 647–51.
Sia S, Lepri A, Ponzecchi P. Axillary brachial plexus block using peripheral nerve stimulator: a comparison between double- and triple-injection techniques. Reg Anesth Pain Med 2001; 26: 499–503.
Partridge BL, Katz J, Benirschke K. Functional anatomy of the brachial plexus sheath: implications for anesthesia. Anesthesiology 1987; 66: 743–7.
Author information
Authors and Affiliations
Corresponding author
Additional information
Funded by: Physician Services Incorporated and Canadian Anesthesiologists’ Society, Smiths Medical Canada Ltd. Canadian Research Award in Pain Research and/or Regional Anesthesia.
Equipment support by: Philips Medical System.
An erratum to this article is available at http://dx.doi.org/10.1007/BF03022334.
Rights and permissions
About this article
Cite this article
Chan, V.W.S., Perlas, A., McCartney, C.J.L. et al. Ultrasound guidance improves success rate of axillary brachial plexus block. Can J Anesth 54, 176–182 (2007). https://doi.org/10.1007/BF03022637
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03022637