
Abstract
Purpose
To describe cardiovascular collapse during a cemented hip hemiarthroplasty in a patient who, despite a successful cardiopulmonary resuscitation, remained in a persistent vegetative state due to cerebral fat embolism diagnosed by magnetic resonance imaging (MRI).
Clinical features
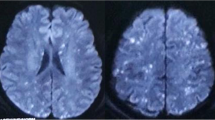
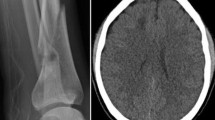
A 75-yr-old woman with no medical history underwent cemented hip hemiarthroplasty under spinal anesthesia for a right femoral neck fracture. Shortly after insertion of the prosthesis, a sudden oxygen desaturation, hypotension, bradycardia, and cardiac arrest occurred. The patient was successfully resuscitated, but did not regain consciousness. The patient developed highgrade fever, thrombocytopenia, anemia, and oliguria. MRI scans of the brain revealed multiple high intensity signals throughout the white matter, the basal ganglia, the cerebellum, and the brain stem. The diagnosis of fat embolism was made on the basis of clinical findings and MRI images. Although her cardiorespiratory status improved over the next week, the patient remained in a persistent vegetative state.
Conclusion
When fat embolism is suspected, serial MRI scans of the brain should be performed to diagnose the etiology of cerebral embolism as well as to evaluate the severity of brain damage.
Résumé
Objectif
Décrire le collapsus cardiovasculaire survenu pendant une hémi-arthroplastie de la hanche chez une patiente qui, malgré une réanimation cardiopulmonaire réussie, est demeurée dans un état végétatif persistant à cause d’une embolie graisseuse diagnostiquée grâce à l’imagerie par résonance magnétique.
Éléments cliniques
Une femme de 75 ans, sans antécédents médicaux, a subi une hémi-arthroplastie cimentée de la hanche sous rachianesthésie à la suite d’une fracture du col du fémur. Peu après l’insertion de la prothèse, il y a eu l’apparition soudaine de désaturation en oxygène, d’hypotension, de bradycardie et un arrêt cardiaque. La patiente, réanimée avec succès, n’a pourtant pas repris conscience. Une forte fièvre, une thrombocytopénie, de l’anémie et de l’oligurie se sont développées. L’IRM du cerveau a révélé de multiples signaux de haute intensité dans la matière blanche, les noyaux gris centraux, le cervelet et le tronc cérébral. Les constatations cliniques et les images d’IRM ont conduit au diagnostic d’embolie graisseuse. Même si l’état cardiorespiratoire s’est amélioré au cours de la semaine suivante, la patiente est demeurée dans un état végétatif persistant.
Conclusion
En cas d’embolie graisseuse présumée, une série d’examens d’IRM du cerveau devraient être faits pour découvrir la cause de l’embolie et évaluer la sévérité de la lésion.
Article PDF
Similar content being viewed by others

References
Colonna DM, Kilgus D, Brown W, Challa V, Stump DA, Moody DM. Acute brain fat embolization occurring after total hip arthroplasty in the absence of a patent foramen ovale. Anesthesiology 2002; 96: 1027–9.
Fallon KM, Fuller JG, Morley-Forster P. Fat embolization and fatal cardiac arrest during hip arthroplasty with methylmethacrylate. Can J Anesth 2001; 48: 626–9.
Pietak S, Holmes J, Matthews R, Petrasek A, Porter B. Cardiovascular collapse after femoral prosthesis surgery for acute hip fracture. Can J Anaesth 1997; 44: 198–201.
Sevitt S. Fat embolism in patients with fractured hips. Br Med J 1972; 2: 257–62.
Gresham GA, Kuczynski A, Rosborough D. Fatal fat embolism following replacement arthroplasty for transcervical fractures of femur. Br Med J 1971; 2: 617–9.
Dandy DJ. Fat embolism following prosthetic replacement of the femoral head. Injury 1971; 3: 85–8.
Orsini EC, Richards RR, Mulen JM. Fatal fat embolism during cemented total knee arthroplasty: a case report. Can J Surg 1986; 29: 385–6.
Patterson BM, Healey JH, Cornell CN, Sharrock NE. Cardiac arrest during hip arthroplasty with a cemented long-stem component. J Bone Joint Surg 1991; 73: 271–7.
Dive AM, Dubois PE, Ide C, Bulpa PA, Broka SM, Installe E. Paradoxical cerebral fat embolism: an unusual cause of persistent unconsciousness after orthopedic surgery. Anesthesiology 2002; 96: 1029–31.
Byrick RJ, Korley RE, McKee MD, Schemitsch EH. Prolonged coma after unreamed, locked nailing of femoral shaft fracture. Anesthesiology 2001; 94: 163–5.
Ozelsel TJ, Hein HA, Marcel RJ, Rathjen KW, Ramsay MA, Jackson RW. Delayed neurological deficit after total hip arthroplasty. Anesth Analg 1998; 87: 1209–10.
Satoh H, Kurisu K, Ohtani M, et al. Cerebral fat embolism studied by magnetic resonance imaging, transcranial Doppler sonography, and single photon emission computed tomography: case report. J Trauma 1997; 43: 345–8.
Schemitsch EH, Turchin DC, Anderson GI, Byrick RJ, Mullen JB, Richards RR. Pulmonary and systemic fat embolization after medullary canal pressurization: a hemodynamic and histologic investigation in the dog. J Trauma 1998; 45: 738–42.
Ereth MH, Weber JG, Abel MD, et al. Cemented versus noncemented total hip arthroplasty: embolism hemodynamics, and intrapulmonary shunting. Mayo Clin Proc 1992; 67: 1066–74.
Orsini EC, Byrick RJ, Mullen JB, Kay JC, Waddell JP. Cardiopulmonary function and pulmonary microemboli during arthroplasty using cemented or non-cemented components. J Bone Joint Surg 1987; 69: 822–32.
Byrick RJ, Mullen JB, Mazer CD, Guest CB. Transpulmonary systemic fat embolism. Studies in mongrel dogs after cemented arthroplasty. Am J Respir Crit Care Med 1994; 150: 1416–22.
Urban MK, Sheppard R, Gordon MA, Urquhart BL. Right ventricular function during revision total hip arthroplasty. Anesth Analg 1996; 82: 1225–9.
Herndon JH, Bechtol CO, Crickenberger DP. Fat embolism during total hip replacement. J Bone Joint Surg 1974; 56: 1350–62
Edmonds CR, Barbut D, Hager D, Sharrock NE. Intraoperative cerebral arterial embolization during total hip arthroplasty. Anesthesiology 2000; 93: 315–8.
Sulek CA, Davies LK, Enneking FK, Gearen PA, Lobato EB. Cerebral microembolism diagnosed by transcranial Doppler during total knee arthroplasty. Correlation with transesophageal echocardiography. Anesthesiology 1999; 91: 672–6.
Takahashi M, Suzuki R, Osakabe Y, et al. Magnetic resonance imaging findings in cerebral fat embolism: correlation with clinical manifestations. J Trauma 1999; 46: 324–7.
Kamenar E, Burger PC. Cerebral fat embolism: a neuropathological study of a microembolic state. Stroke 1980; 11: 477–84.
Takahashi S, Higano S, Ishii K, et al. Hypoxic brain damage: cortical laminar necrosis and delayed changes in white matter at sequential MR imaging. Radiology 1993; 189: 449–56.
Arbelaez A, Castillo M, Mukherji SK. Diffusion-weighted MR imaging of global cerebral anoxia. AJNR 1999; 20: 999–1007.
Chalela JA, Wolf RL, Maldjian JA, Kasner SE. MRI identification of early white matter injury in anoxicischemic encephalopathy. Neurology 2001; 56: 481–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sasano, N., Ishida, S., Tetsu, S. et al. Cerebral fat embolism diagnosed by magnetic resonance imaging at one, eight, and 50 days after hip arthroplasty: a case report. Can J Anesth 51, 875–879 (2004). https://doi.org/10.1007/BF03018883
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03018883