
Abstract
Purpose: To determine whether a functional difference exists between the size 2 laryngeal mask airway (LMA)-Classic™ (CLMA) and LMA-Proseal™ (PLMA) in anesthetized children who have received neuromuscular blockade. Airway leak during intermittent positive pressure ventilation (IPPV) and adequacy of fibreoptic laryngeal view were the primary study outcomes.
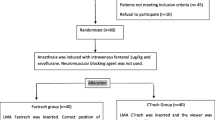
Methods: A randomized, controlled, single-blinded study of 51 ASA I or II children weighing 10–20 kg was undertaken. The anesthetic technique was standardized. Following insertion of the LMA and cuff inflation to 60 cm H2O, we measured oropharyngeal leak pressure and gastric insufflation and leak fraction during IPPV, and evaluated the adequacy of fibreoptic view.
Results: Oropharyngeal leak pressure measured by neck auscultation was higher for the PLMA compared to the CLMA (23.7vs 16.5 cm H2O,P=0.009) but, when measured by the inspiratory hold maneuver was not significantly different (24.8vs 20.3 cm H2O, respectively,P=0.217). Leak fraction values were similar for the CLMA and the PLMA (21.2%.vs 13.3%, respectively,P=0.473). A satisfactory view of the larynx was obtained more frequently in the PLMA group (21/25vs 10/25,P=0.003). Gastric insufflation during leak determination was more common with the CLMA (12/26vs 2/25 CLMAvs PLMA, respectively,P=0.006).
Conclusion: In children undergoing IPPV with neuromuscular blockade, the size 2 PLMA is associated with a higher leak pressure by auscultation and less gastric insufflation compared to the CLMA. Leak pressures assessed by manometric stability are similar with these two devices. The improved fibreoptic view of the larynx through the PLMA may be advantageous for bronchoscopy.
Résumé
Objectif: Déterminer s’il existe une différence fonctionnelle entre les masques laryngés (LMA)-Classic™ (CLMA) et LMA-ProSeal™ (PLMA) de taille 2 chez les enfants anesthésiés lors d’un bloc neuromusculaire. Les fuites du masque pendant la ventilation à pression positive intermittente (VPPI) et une bonne vision laryngée par fibre optique constituaient les résultats principaux recherchés par cette étude.
Méthode: Une étude randomisée contrôlée en aveugle portant sur 51 enfants ASA I ou II et pesant entre 10 et 20 kg a été menée. La technique anesthésique utilisée a été standardisée. Après avoir inséré le LMA et gonflé le ballonnet à 60 cm H2O, nous avons mesuré la pression de fuite oropharyngienne, l’insufflation gastrique et la fraction de fuite pendant la VPPI, et avons évalué la qualité de la vision par fibre optique.
Résultats: La pression de fuite oropharyngienne mesurée par auscultation du cou était plus élevée lors de l’utilisation du PLMA que du CLMA (23,7 vs 16,5 cm H2O, P=0,009) ; toutefois, lorsque celle-ci a été mesurée par manœuvre de retenue respiratoire, il n’y a pas eu de différence significative (24,8 vs 20,3 cm H2O, respectivement, P=0,217). Les valeurs de fraction de fuite étaient semblables avec le CLMA et le PLMA (21,2 % vs 13,3 %, respectivement, P=0,473). Une vision satisfaisante du larynx a été plus fréquemment obtenue dans le groupe PLMA (21/25 vs 10/25, P=0,003). L’insufflation gastrique pendant la détermination de la fuite a été plus fréquemment observée dans le groupe CLMA (12/26 vs 2/25 CLMA vs PLMA, respectivement, P=0,006).
Conclusion: Chez les enfants subissant une VPPI lors d’un bloc neuromusculaire, le PLMA de taille 2 est associé à une pression de fuite plus élevée par auscultation et moins d’insufflation gastrique par rapport à une utilisation du CLMA. Les pressions de fuite évaluées par stabilité manométrique sont semblables avec les deux appareils. Une vision par fibre optique améliorée du larynx avec le PLMA pourrait s’avérer utile pour la bronchoscopie.
Article PDF
Similar content being viewed by others


References
Brambrink AM, Meyer RR, Kretz FJ. Management of pediatric airway-anatomy, physiology and new developments in clinical practice (German). Anaesthesiol Reanim 2003; 28: 144–51.
Park C, Bahk JH, Ahn WS, Do SH, Lee KH. The laryngeal mask airway in infants and children. Can J Anesth 2001; 48: 413–7.
Brimacombe J, Keller C, Boehler M, Puhringer F. Positive pressure ventilation with the ProSeal versus classic laryngeal mask airway: a randomized, crossover study of healthy female patients. Anesth Analg 2001; 93: 1351–3.
Braun U, Zerbst M, Fullekrug B, et al. A comparison of the Proseal laryngeal mask to the standard laryngeal mask on anesthesized, non-relaxed patients (German). Anasthesiol Intensivmed Notfallmed Schmerzther 2002; 37: 727–33.
Agro F, Antonelli S, Mattei A. The proseal LMA: preliminary data. Br J Anaesth 2001; 86: 601–2.
Brimacombe J, Keller C, Fullekrug B, et al. A multicenter study comparing the ProSeal and Classic laryngeal mask airway in anesthetized, nonparalyzed patients. Anesthesiology 2002; 96: 289–95.
Stix MS, Borromeo CJ, O’Connor CJ Jr. Esophageal insufflation with normal fiberoptic positioning of the ProSeal laryngeal mask airway. Anesth Analg 2002; 94: 1036–9.
Elwood T, Cox RG. Laryngeal mask insertion with a laryngoscope in paediatric patients. Can J Anaesth 1996; 43: 435–7.
Goudsouzian NG, Denman W, Cleveland R, Shorten G. Radiologic localization of the laryngeal mask airway in children. Anesthesiology 1992; 77: 1085–9.
Keller C, Brimacombe J. Mucosal pressure and oropharyngeal leak pressure with the ProSeal versus laryngeal mask airway in anaesthetized paralysed patients. Br J Anaesth 2000; 85: 262–6.
Keller C, Brimacombe JR, Keller K, Morris R. Comparison of four methods for assessing airway sealing pressure with the laryngeal mask airway in adult patients. Br J Anaesth 1999; 82: 286–7.
Berman LS, Banner MJ, Blanch PB, Widner LR. A new pediatric respiratory monitor that accurately measures imposed work of breathing: a validation study. J Clin Monit 1995; 11: 14–7.
Jackson EA, Coates AL, Gappa M, Stocks J. In vitro assessment of infant pulmonary function equipment. Pediatr Pulmonol 1995; 19: 205–13.
Tsujimura Y. Downfolding of the epiglottis induced by the laryngeal mask airway in children: a comparison between two insertion techniques. Paediatr Anaesth 2001; 11: 651–5.
Goldmann K, Roettger C, Wulf H. The size 1 1/2 ProSeal laryngeal mask airway in infants: a randomized, crossover investigation with the Classic laryngeal mask airway. Anesth Analg 2006; 102: 405–10.
Goldmann K, Jakob C. Size 2 ProSeal laryngeal mask airway: a randomized, crossover investigation with the standard laryngeal mask airway in paediatric patients. Br J Anaesth 2005; 94: 385–9.
Goldmann K, Jakob C. A randomized crossover comparison of the size 2 1/2 laryngeal mask airway ProSeal versus laryngeal mask airway-Classic in pediatric patients. Anesth Analg 2005; 100: 1605–10.
Shimbori H, Ono K, Miwa T, Morimura N, Noguchi M, Hiroki K. Comparison of the LMA-ProSeal and LMA-Classic in children. Br J Anaesth 2004; 93: 528–31.
Lopez-Gil M, Brimacombe J, Garcia G. A randomized non-crossover study comparing the ProSeal and Classic laryngeal mask airway in anaesthetized children. Br J Anaesth 2005; 95: 827–30.
Finholt DA, Henry DB, Raphaely RC. Factors affecting leak around tracheal tubes in children. Can Anaesth Soc J 1985; 32: 326–9.
Goldmann K, Hoch N, Wulf H. Influence of neuromuscular blockade on the airway leak pressure of the ProSeal laryngeal mask airway (German). Anasthesiol Intensivmed Notfallmed Schmerzther 2006; 41: 228–32.
Lopez-Gil M, Brimacombe J, Keller C. A comparison of four methods for assessing oropharyngeal leak pressure with the laryngeal mask airway (LMA) in paediatric patients. Paediatr Anaesth 2001; 11: 319–21.
Brimacombe J, Keller C. The ProSeal laryngeal mask airway: a randomized, crossover study with the standard laryngeal mask airway in paralyzed, anesthetized patients. Anesthesiology 2000; 93: 104–9.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosures: Vitaid Ltd provided LMA-Proseal™ devices for the study. The study was supported by The Division of Pediatric Anesthesia, Alberta Children’s Hospital, Calgary, Alberta, Canada.
Rights and permissions
About this article
Cite this article
Lardner, D.R.R., Cox, R.G., Ewen, A. et al. Comparison of laryngeal mask airway (LMA)-Proseal™ and the LMA-Classic™ in ventilated children receiving neuromuscular blockade. Can J Anaesth 55, 29–35 (2008). https://doi.org/10.1007/BF03017594
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03017594