
Abstract
Purpose
“To evaluate the use of inhalational induction followed by intubation through the intubating laryngeal mask (ILM) for patients with severe ankylosing spondylitis undergoing elective surgery who prefer airway management under anesthesia.
Methods
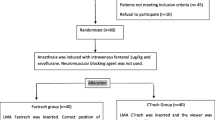
Nine patients undergoing a total of II procedures were enrolled in the study. Fentanyl 2μg·kg−1 midazolam 0.035 mg·kg−1 and sevoflurane in oxygen 100% were used for induction. The ILM was inserted when the end-tidal sevoflurane concentration reached 3%. After an effective airway was established, atracurium 0.5 mg·kg−1 was given. A polyvinyl chloride tube in the reversed position using a blind technique was used to intubate the trachea.
Results
The ILM provided an effective airway on 11/11 occasions at the first attempt. Intubation was successful at the first attempt on 7/11 occasions, at the second attempt on 2/11 and at the third attempt in 1/11. Intubation failed in one patient. The mean (range) minimal oxygen saturation was 99.4% (97–100%). There were no problems with ILM removal.
Conclusion
Inhalational induction followed by ILM insertion and blind intubation is a reasonable option in patients with severe ankylosing spondylitis undergoing elective surgery who prefer airway management under anesthesia.
Résumé
Objectif
Évaluer l’utilisation de l’induction par inhalation suivie de l’intubation au travers du masque laryngé d’intubation (MLI) chez des patients qui présentent une spondylarthrite ankylosante sévère, qui doivent subir une intervention non urgente, mais qui préfèrent une intubation sous anesthésie.
Méthode
Neuf patients, admis pour 11 interventions au total, ont été recrutés pour participer à l’étude. On a utilisé 2μg·kg−1 de fentanyl, 0,035 mg·kg−1 de midazolam et du sévoflurane dans de l’oxygène à 100 % pour l’induction anesthésique. On a ensuite inséré le MLI quand la concentration de sévoflurane de fin d’expiration a atteint 3 %. Après avoir assurer la liberté des voies respiratoires, on a administré 0,5 mg·kg−1 d’atracurium. On a utilisé un tube endotrachéal de chlorure de polyvinyle en position renversée pour réaliser l’intubation endotrachéale à l’aveugle.
Résultats
Le MLI a permis une perméabilité efficace des voies aériennes 11/11 fois au premier essai. L’intubation a été réussie au premier essai dans 7/11 cas, au second essai dans 2/11 cas et au troisième, dans un cas. L’intubation a été un échec chez un patient. La saturation minimale moyenne en oxygène (intervalle) a été de 99,4 % (97–100 %). Le MLI a été retiré sans difficulté.
Conclusion
L’induction par inhalation suivie de l’insertion d’un MLI et d’une intubation à l’aveugle apparaît comme une option possible chez des patients atteints de spondylarthrite ankylosante sévère qui préfèrent une intubation sous anesthésie.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Defalque RJ, Hyder ML. Laryngeal mask airway in severe cervical ankylosis. Can J Anaesth 1997; 44: 305–7.
Williams PJ, Bailey PM. Management of failed oral fibreoptic intubation with laryngeal mask airway insertion under topical anaesthesia (Letter). Can J Anaesth 1993; 40: 287
Steib A, Seller JP, Lleu JC, Otteni JC. Difficult intubation managed by laryngeal mask and fibroscopy (French). Ann Fr Anesth Reanim 1992; 11: 601–3.
Jun JH, Seung LS, Cho SY, Suh JK. Laryngeal mask airway — endotracheal intubation with laryngeal mask airway and fibreoptic bronchoscope. J Kor Soc Anesthesiol 1993; 26: 1029–34.
Wallace EJ, Chung F. General anesthesia in a patient with an enlarged saber sheath trachea. Anesthesiology 1998; 88: 527–9.
Dimitriou V, Voyagis G, Hrimacombe J. Flexible lightwand-guided intubation through the ILM (Letter). Acta Anaesthesiol Scand 2001; 45: 263–4.
Chadd GD, Ackers JWL, Bailey PM. Difficult intubation aided by the laryngeal mask airway (Letter). Anaesthesia 1989; 44: 1015.
Lu P-P, Yang C-H, Ho ACY, Shyr M-H. The intubating LMA: a comparison of insertion techniques with conventional tracheal tubes. Can J Anesth 2000; 47: 849–53.
Maltby JR, Loken RG, Beriault MT, Archer DP. Laryngeal mask airway with mouth opening less than 20 mm. Can J Anaesth 1995; 42: 1140–2.
Brimacombe J, Keller C, Weidmann K. Limited mouth opening and the intubating laryngeal mask (Letter). Can J Anaesth 1999; 46: 807–8.
Aziz ES, Thompson AR, Baer S. Difficult laryngeal mask insertion in a patient with Forestier’s disease (Letter). Anaesthesia 1995; 50: 370.
Ishimura H, Minami K, Sata T, Shigematsu A, Kadoya T. Impossible insertion of the laryngeal mask airway and oropharyngeal axes. Anesthesiology 1995; 83: 867–9.
Asai T, Wagle AU, Stacey M. Placement of the intubating laryngeal mask is easier than the laryngeal mask during manual in-line neck stabilization. Br J Anaesth 1999; 82: 712–4.
Lucas DN, Tentis SM. A comparison of the intubating laryngeal mask tracheal tube with a standard tracheal tube for fibreoptic intubation. Anaesthesia 2000; 55: 358–61.
Kihara S, Watanabe S, Taguchi N, Suga A, Brimacombe JR. Tracheal intubation with the Macintosh laryngoscope versus intubating laryngeal mask airway in adults with normal airways. Anaesth Intens Care 2000; 28: 281–6.
Rocchiccioli C, Blumen M, Chabolle F, Fischler M. Successful use of LMA Fastrach™ (FT) in patients with obstructive sleep apnea syndrome and predictive signs of difficult airway. Anesthesiology 2000; 93: A1112 (abstract).
King C, Street MK. Twelfth cranial nerve paralysis following use of a laryngeal mask airway. Anaesthesia 1994; 49: 786–7.
Smigovec E, Sakic K, Tripkovic B. The laryngeal mask—news in orthopedic anesthesia (Roman). Lijec Vjesn 1993; 115: 166–9.
Pothmann W, Eckert S, Fullekrug B. Use of the laryngeal mask in difficult intubation (German). Anaesthesist 1993; 42: 644–7.
Kinirons B, Dwyer R. Renal transplantation in a patient with ankylosing spondylitis. Br J Hosp Med 1996; 56: 298.
Forestier J, Rotes Querol J. Senile ankylosing hyperostosis of the spine. Annals of Rheumatic Disease 1950; 9: 321–30.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lu, PP., Brimacombe, J., Ho, A.C.Y. et al. The intubating laryngeal mask airway in severe ankylosing spondylitis. Can J Anaesth 48, 1015–1019 (2001). https://doi.org/10.1007/BF03016593
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016593