
Abstract
Purpose
To compare the risk-adapted approach with ondansetron against ondansetron plus dexamethasone to prevent postoperative nausea and vomiting (PONV) in a randomized clinical trial.
Methods
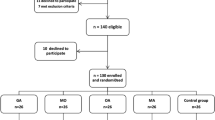
460 patients scheduled for elective surgery were enrolled in this prospective study and stratified according to a simplified risk score for PONV. Patients having no or one risk factor were considered at low risk (group L) and did not receive study medication. Those with two to four risk factors were considered high risk and were randomized to receive 4 mg ondansetron plus placebo (group H-O) or 4 mg ondansetron plus 8 mg dexamethasone (group H-OD). Incidence and intensity of PONV were observed for 24 hr after surgery. Data were analyzed with Fisher’s exact or Student’s t tests;P < 0.05 was considered statistically significant.
Results
The incidence of PONV was 9% in group L (n = 87), 31% in those receiving ondansetron (group H-O,n = 185), and 22% in those receiving both drugs (group H-OD,n = 181). The incidence of PONV was significantly smaller in both high-risk groups than predicted without treatment (P < 0.001). While the incidence of PONV failed statistical significance between the two intervention groups (P = 0.08), the mean number of episodes of PONV and the mean maximal intensity of each episode of PONV were lower in group H-OD (P = 0.03 andP = 0.01, respectively). Patients of group H-OD required less antiemetic rescue therapy (P = 0.004). Conclusions: Ondansetron plus dexamethasone prevents PONV more effectively than ondansetron alone in patients at high risk for PONV.
Résumé
Objectif
Comparer l’approche adaptée au risque avec ondansétron ou avec ondansétron et dexaméthasone pour prévenir les nausées et vomissements postopératoires (NVPO) dans une étude clinique randomisée.
Méthode
L’étude prospective a porté sur 460 patients, devant subir une intervention chirurgicale réglée, qui ont été stratifiés selon un score de risque simplifié de NVPO. Les patients ont été considérés à faible risque (groupe F) s’ils n’avaient aucun ou un facteur de risque et n’ont pas reçu la médication à l’étude. S’ils avaient de deux à quatre facteurs de risque, on les considérait à haut risque et ils recevaient au hasard 4 mg d’ondansétron plus un placebo (groupe H-O) ou 4 mg d’ondansétron plus 8 mg de dexaméthasone (groupe H-OD). L’incidence et l’intensité des NVPO ont été observées pendant 24 h après l’opération. Les données ont été analysées par les tests exact de Fisher ou t de Student ; P < 0,05 était statistiquement significatif.
Résultats
L’incidence de NVPO a été de 9 % dans le groupe F (n = 87), 31 % avec l’ondansétron (groupe H-O, n = 185) et 22 % avec les deux médicaments (groupe H-OD, n = 181). L’incidence de NVPO a été significativement plus basse dans les deux groupes à haut risque que ce qui avait été prédit sans traitement (P < 0,001). Même si l’incidence de NVPO n’était pas statistiquement significative entre les deux groupes expérimentaux (P = 0,08), le nombre moyen d’épisodes de NVPO et l’intensité maximale moyenne de chacun ont été plus faibles dans le groupe H-OD (P = 0,03 et P = 0,01, respectivement). Les patients du groupe H-OD ont demandé moins d’antiémétiques de secours P = 0,004).
Conclusion
L’ondansétron plus la dexaméthasone préviennent les NVPO plus efficacement que l’ondansétron seul chez des patients à haut risque de NVPO.
Article PDF
Similar content being viewed by others


References
Frighetto L, Loewen PS, Dolman J, Marra CA. Costeffectiveness of prophylactic dolasetron or droperidol vs rescue therapy in the prevention of PONV in ambulatory gynecologic surgery. Can J Anesth 1999; 46:536–43.
Hill RP, Lubarsky DA, Phillips-Bute B, et al. Cost-effectiveness of prophylactic antiemetic therapy with ondansetron, droperidol, or placebo. Anesthesiology 2000; 92:958–67.
Scuderi PE, James RL, Harris L, Mims GR III. Antiemetic prophylaxis does not improve outcomes after outpatient surgery when compared to symptomatic treatment. Anesthesiology 1999; 90:360–71.
Tramer MR. A rational approach to the control of postoperative nausea and vomiting: evidence from systematic reviews. Part I. Efficacy and harm of antiemetic interventions, and methodological issues. Acta Anaesthesiol Scand 2001; 45:4–13.
Gan TJ, Meyer T, Apfel CC, et al. Consensus guidelines for managing postoperative nausea and vomiting. Anesth Analg 2003; 97:62–71.
Tramer M, Moore A, McQuay H. Propofol anaesthesia and postoperative nausea and vomiting: quantitative systematic review of randomized controlled studies. Br J Anaesth 1997; 78:247–55.
Rajeeva V, Bhardwaj N, Batra YK, Dhaliwal LK. Comparison of ondansetron with ondansetron and dexamethasone in prevention of PONV in diagnostic laparoscopy. Can J Anesth 1999; 46:40–4.
Shende D, Bharti N, Kathirvel S, Madan R. Combination of droperidol and ondansetron reduces PONV after pediatric strabismus surgery more than single drug therapy. Acta Anaesthesiol Scand 2001; 45:756–60.
Ahmed AB, Hobbs GJ, Curran JP. Randomized, placebo- controlled trial of combination antiemetic prophylaxis for day-case gynaecological laparoscopic surgery. Br J Anaesth 2000; 85:678–82.
Henzi I, Walder B, Tramer MR. Dexamethasone for the prevention of postoperative nausea and vomiting: a quantitative systematic review. Anesth Analg 2000; 90:186–94.
Eberhart LH, Morin AM, Georgieff M. Dexamethasone for prophylaxis of postoperative nausea and vomiting. A meta-analysis of randomised controlled studies (German). Anaesthesist 2000; 49:713–20.
Apfel CC, Laara E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting. Conclusions from cross-validations between two centers. Anesthesiology 1999; 91:693–700.
Apfel CC, Kranke P, Eberhart LH, Roos A, Roewer N. Comparison of predictive models for postoperative nausea and vomiting. Br J Anaesth 2002; 88:234–40.
Pierre S, Benais H, Pouymayou J. Apfel’s simplified score may favourably predict the risk of postoperative nausea and vomiting. Can J Anesth 2002; 49:237–42.
Apfel CC, Roewer N, Korttila K. How to study postoperative nausea and vomiting. Acta Anaesthesiol Scand 2002; 46:921–8.
Apfel CC, Korttila K, Abdalla M, et al. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med 2004; 350:2441–51.
Visser K, Hassink EA, Bonsel GJ, Moen J, Kalkman CJ. Randomized controlled trial of total intravenous anesthesia with propofol versus inhalation anesthesia with isoflurane-nitrous oxide. Postoperative nausea and vomiting and economic analysis. Anesthesiology 2001; 95:616–26.
Aspinall RL, Goodman NW. Denial of effective treatment and poor quality of clinical information in placebo controlled trials of ondansetron for postoperative nausea and vomiting: a review of published trials. BMJ 1995; 311:844–6.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure: This study was funded by GlaxoSmithKline, Germany.
Rights and permissions
About this article
Cite this article
Rüsch, D., Eberhart, L., Biedler, A. et al. Prospective application of a simplified risk score to prevent postoperative nausea and vomiting. Can J Anesth 52, 478–484 (2005). https://doi.org/10.1007/BF03016526
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016526