
Abstract
Purpose
To assess the effect of cricoid pressure on the positioning of and ventilation through the laryngeal mask airway (LMA).
Methods
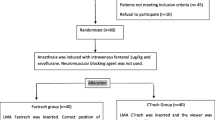
In a double-blind, randomized design, the LMA was inserted with (CP[+] group, n = 20) or without double-handed cricoid pressure (CP[−] group, n = 20). Ventilation through the LMA was assessed by measuring expiratory tidal volume and judged as adequate when a mean expiratory tidal volume of ≥10 ml · kg−1 could be obtained. The LMA position was examined by fibreoscopy. The position of the mask relative to the cricoid cartilage and the cervical spine was radiologically examined (n = 10 in each group).
Results
Ventilation was adequate in all patients in the CP[−] group but in only five patients (25%) of the CP[+] group (P < 0.001). The glottis was visible fibreoptically below the mask aperture in all patients in the CP[−] group, but in only three patients in the CP[+] group (P < 0.001). Fibreoscopy showed that the mask was not inserted far enough in the remaining 17 patients of the CP[+] group. The reason for unsuccessful ventilation in the CP[+] group was excessive gas leakage (n = 2) and/or partial or complete airway obstruction (n = 13), which was noted fibreoptically. The radiographs showed that the tip of the mask in the CP[−] group was located below the level of the cricoid cartilage (C6 or C7 vertebra). The mask tip in the CP[+] group was above this level (C4 or C5 vertebra) (P < 0.01).
Conclusion
Cricoid pressure impedes positioning of and ventilation through the LMA.
Résumé
Objectif
Vérifier l’influence de la pression cricoïdienne sur la ventilation au masque laryngé (ML) et son positionnement.
Méthodes
Au cours de cette étude aléatoire et en double aveugle, le LM a été inséré avec (groupe CP[+], n = 20) ou sans pression cricoïdienne manuelle (groupe CP[−], n = 20). La ventilation par masque laryngée était évaluée par la mesure du volume courant expiré et jugée suffisante lorsqu’on obtenait un volume minute expiré ≥10 ml · kg−1. La position du ML était vérifiée par fibroscopie. Chez dix patients de chaque groupe, l’examen radiologique a déterminé la position du ML relativement au cartilage cricoïde et à la colonne cervicale.
Résultats
La ventilation a été adéquate chez tous les patients du groupe CP[−] mais chez seulement cinq (25%) du groupe CP[+] (P < 0,001). La glotte était visible par fibroscopie sous l’ouverture du masque chez tous les patients du groupe CP[−], mais chez seulement trois du groupe CP[+]. La fibroscopie a montré que le masque n ’était pas inséré assez profondément chez les 17 autres patients du groupe CP[+]. Cet échec ventilatoire dans le groupe CP[+] était causé par une fuite de gaz exagérée (n = 2) ou/et par l’obstruction des voies aériennes partielle ou complète (n = 13), vérifiée par fibroscopie. Les radiographies ont révélé que la pointe du masque dans le groupe CP[−] était située sous le niveau du cartilage cricoïde (C6 ou C7). Dans le groupe CP[+], la pointe du masque était située à un niveau plus élevé (C4 ou C5, P < 0,01).
Conclusion
La pression cricoïdienne nuit et à la ventilation au masque laryngé et a son positionnement.
Article PDF
Similar content being viewed by others


References
Brain AIJ, McGhee TD, McAteer EJ, Thomas A, Abu-Saad MAW, Bushman JA. The laryngeal mask airway. Development and preliminary trials of a new type of airway. Anaesthesia 1985; 40: 356–61.
Maltby JR, Loken RG, Watson NC. The laryngeal mask airway: clinical appraisal in 250 patients. Can J Anaesth 1990; 37: 509–13.
Brain AIJ. Three cases of difficult intubation overcome by the laryngeal mask airway. Anaesthesia 1985; 40: 353–5.
Asai T, Morris S. The laryngeal mask airway: its features, effects and role. Can J Anaesth 1994; 41: 930–60.
Fisher JA, Ananthanarayan C, Edelist G. Role of the laryngeal mask in airway management (Editorial). Can J Anaesth 1992; 39: 1–3.
McClune S, Regan M, Moore J. Laryngeal mask airway for Caesarean section. Anaesthesia 1990; 45: 227–8.
Priscu V, Priscu L, Soroker D. Laryngeal mask for failed intubation in emergency Caesarean section (Letter). Can J Anaesth 1992; 39: 893.
Heath ML, Allagain J. Intubation through the laryngeal mask. A technique for unexpected difficult intubation. Anaesthesia 1991; 46: 545–8.
Brimacombe J, White A, Berry A. Effect of cricoid pressure on ease of insertion of the laryngeal mask airway. Br J Anaesth 1993; 71: 800–2.
Ansermino JM, Blogg CE. Cricoid pressure may prevent insertion of the laryngeal mask airway. Br J Anaesth 1992; 69: 465–7.
Asai T, Barclay K, Power I, Vaughan RS. Cricoid pressure impedes placement of the laryngeal mask airway and subsequent tracheal intubation through the mask. Br J Anaesth 1994; 72: 47–51.
Asai T, Barclay K, Power I, Vaughan RS. Cricoid pressure impedes placement of the laryngeal mask airway. Br J Anaesth 1995; 74: 521–5.
Asai T, Morris S. The role of the laryngeal mask for failed tracheal intubation in the patient with a “full stomach” (Letter). Anesth Analg 1994; 78: 817–8.
Brimacombe J, Berry A. The role of the laryngeal mask for failed tracheal intubation in the patient with a “full stomach” (Letter). Anesth Analg 1994; 78: 818–9.
Asai T. Difficulty in assessing the correct position of the laryngeal mask airway (Letter). Br J Anaesth 1994; 72: 366.
Nandi PR, Nunn JF, Charlesworth CH, Taylor SJ. Radiological study of the laryngeal mask. Eur J Anaesthesiol Suppl 1991; 4: 33–9.
Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J 1985; 32: 429–34.
Samsoon GLT, Young JRB. Difficult tracheal intubation: a retrospective study. Anaesthesia 1987; 42: 487–90.
Brain AIJ. The Intavent Laryngeal Mask. Instruction Manual, 2nd ed. England: Intavent, 1993.
Crowley DS, Giesecke AH. Bimanual cricoid pressure (Letter). Anaesthesia 1990; 45: 588–9.
Aoyama K, Takenaka I, Sata T, Shigematsu A. The triple airway manoeuvre for insertion of the laryngeal mask airway in paralyzed patients. Can J Anaesth 1995; 42: 1010–6.
Brain AIJ. Laryngeal mask misplacement —causes, consequences and solutions (Letter). Anaesthesia 1992; 47: 531–2.
Williams PL, Warwick R, Dyson M, Bannister LH. Gray’s Anatomy, 37th ed. New York: Churchill Livingstone, 1989.
Asai T, Barclay K, Power I, Vaughan RS. Cricoid pressure and the LMA: efficacy and interpretation (Letter). Br J Anaesth 1994; 73: 863–5.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Aoyama, K., Takenaka, I., Sata, T. et al. Cricoid pressure impedes positioning and ventilation through the laryngeal mask airway. Can J Anaesth 43, 1035–1040 (1996). https://doi.org/10.1007/BF03011906
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03011906