
Abstract
Introduction: Postoperative radiotherapy (PR) has been recommended in patients with advanced head and neck melanomas to improve regional control. This study examined the incidence of cervical recurrence among patients who did not receive PR after surgical management of nodepositive head and neck melanomas.
Methods: A computerized search of a database listing more than 10,000 patients with melanoma prospectively acquired between 1971 and 1998 identified 217 patients with pathologically positive nodes who had undergone regional lymph node dissection (RLND). Of these patients, 21 had received PR and 196 had not.
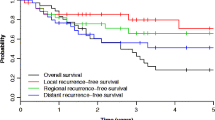
Results: Median follow-up after RLND was 20 months for nonsurvivors and 32 months for survivors. The overall incidence of cervical recurrence was 14% (27/196). The 5-year cervical recurrence-free survival rate was 83%. Five-year cervical recurrence-free survival rates were 69% vs. 87% for patients with vs. without extranodal disease (P=.004), 96% vs. 81% for patients with nonpalpable vs. palpable nodes (P=.0761), and 82% vs. 91% for patients with one to three positive nodes vs. more than three positive nodes (P=.256). Multivariate analysis, which included the timing of nodal disease presentation and the effect of systemic adjuvant therapy, identified extranodal disease as the only independent predictor of cervical recurrence (P=.034). Cervical recurrence was significantly related to the subsequent occurrence of distant relapse.
Conclusions: The low incidence of cervical recurrence after RLND in patients with node-positive head and neck melanomas does not justify the routine use of PR. The only subset of patients who may benefit from PR are those with extranodal disease.
Similar content being viewed by others


References
Byers RM. The role of modified neck dissection in the treatment of cutaneous melanoma of the head and neck.Arch Surg 1986;121:1338–41.
Calabro A, Singletary SE, Balch CM. Patterns of relapse in 1001 consecutive patients with melanoma nodal metastases.Arch Surg 1989;124:1051–5.
Singletary SE, Byers RM, Shallenberger R, et al. Prognostic factors in patients with regional cervical nodal metastases from cutaneous malignant melanoma.Am J Surg 1986;152:371–5.
O’Brien CJ, Gianoutsos MP, Morgan MJ. Neck dissection for cutaneous malignant melanoma.World J Surg 1992;16:222–6.
Santini H, Byers RM, Wolf PF. Melanoma metastatic to cervical and parotid nodes from an unknown primary site.Am J Surg 1985;150:510–12.
Ang KK, Byers RM, Peters LJ, et al. Regional radiotherapy as adjuvant treatment for head and neck malignant melanoma.Arch Otolaryngol Head Neck Surg 1990;116:169–72.
Ang KK, Peters LJ, Weber RS, et al. Postoperative radiotherapy for cutaneous melanoma of the head and neck region.Int J Radiat Oncol Biol Phys 1994;30:795–8.
O’Brien CJ, Petersen-Schaefer K, Stevens GN, et al. Adjuvant radiotherapy following neck dissection and parotidectomy for metastatic malignant melanoma.Head Neck 1997;19:589–94.
Corry J, Smith JG, Bishop M, et al. Nodal radiation therapy for metastatic melanoma.Int J Radiat Oncol Biol Phys 1999;44:1065–9.
Burmeister BH, Smithers BM, Poulsen M, et al. Radiation therapy for nodal disease in malignant melanoma.World J Surg 1995;19:369–71.
Lee RJ, Gibbs JF, Proulx GM, et al. Nodal basin recurrence following lymph node dissection for melanoma: implications for adjuvant radiotherapy.Int J Radiat Oncol Biol Phys 2000;46:467–74.
Creagan ET, Cupps RE, Ivins JC, et al. Adjuvant radiation therapy for regional nodal metastases from malignant melanoma.Cancer 1978;42:2206–10.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shen, P., Wanek, L.A. & Morton, D.L. Is adjuvant radiotherapy necessary after positive lymph node dissection in head and neck melanomas?. Ann Surg Oncol 7, 554–559 (2000). https://doi.org/10.1007/BF02725332
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02725332