
Abstract
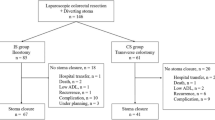
The need for protective transverse colostomy in low anterior resection using the EEA stapler was tested in a randomized series of 50 patients, half of whom received peroperative protective colostomy. Gastrografin® enema, on the tenth postoperative day showed a leakage frequency of 30 per cent in both groups. Clinical leakage was noted in 4 per cent (one patient) in the colostomy group and 12 per cent (three patients) in the noncolostomy group. Protective colostomy was followed by stenosis in nine instances, compared with only two in the noncolostomy group (2α=0.05). Routine protective colostomy should not be used in low anterior resection when the EEA stapling instrument is used. The occasional clinical leakage, which may appear in the postoperative period, can be revealed by close observation and successfully treated by an emergency colostomy. The majority of patients with anterior resection of the rectum, therefore, can be spared the inconvenience and cost of temporary colostomy.
Similar content being viewed by others


References
Goligher JC, Graham NG, De Dombal FT. Anastomotic dehiscence after anterior resection of rectum and sigmoid. Br J Surg 1970;57:109–18.
Morgenstern L, Yamakawa T, Ben-Shoshan M, Lippman H. Anastomotic leakage after low colonic anastomosis: clinical and experimental aspects. Am J Surg 1972;123:104–9.
Elliott TE, Albertazzi VJ, Danto LA. Stenosis after stapler anastomosis. Am J Surg 1977;133:750–1.
Goligher JC Surgery of the anus, rectum and colon. 3rd ed. London: Bailliére Tindall, 1975:714.
Goligher JC, Lee PW, Simpkins KC, Lintott DJ. A controlled comparison of one- and two-layer techniques of suture for high and low colorectal anastomoses. Br J Surg 1977; 64;609–14.
Kirkegaard P. A new technique for low anterior resection of the rectum: preliminary results with a circular stapling instrument for anastomosis. Dan Med Bull 1978;25:235–7.
Dukes CE. The classification of cancer of the rectum. J Pathol Bacteriol 1932;35:323–32.
Ling L, Broomé A, Rydén S. Low anterior resection using stapling instrument. Acta Chir Scand 1979;145:487–9.
Goligher JC, Lee PW, Macfie J, Simpkins KC, Lintott DJ. Experience with the Russian model 249 suture gun for anastomosis of the rectum. Surg Gynecol Obstet 1979;148: 517–24.
Thiede A, Jostarndt L, Troidl H, Poser HL, Bertz U, Hamelmann H. Der Wert der zirkularen maschinellen Colon- und Rectumanastomose (EEA). Eine prospektive Studie an 91 Patienten. Chirurg 1981;52:30–5.
Sharefkin J, Joffe N, Silen W, Fromm D. Anastomotic dehiscence after low anterior resection of the rectum. Am J Surg 1978;135:519–23.
Beart RW Jr, Kelly KA. Randomized prospective evaluation of the EEA stapler for colorectal anastomoses. Am J Surg 1981;141:143–7.
Hermanek P, Gall FP, Der aborale Sicherheitsabstand bei der sphinctererhaltenden Rectumresektion. Chirurg 1981;52:25–9.
Goliger JC Surgery of the anus, rectum and colon. London: Bailliere Tindall, 1975:742.
Schumann J. Die postoperative Anastomosenstenose nach Kontinenzresektion des Sigmas und des Rektums—ein vermeidbares oder schicksalhaftes Ereignis? Zentralbl Chir 1978;103:1247–55.
Smith LE. Anastomosis with EEA stapler after anterior colonic resection. Dis Colon Rectum 1981;24:236–42.
Samhouri F, Grodsinsky C. The morbidity and mortality of colostomy closure. Dis Colon Rectum 1979;22:312–4.
Author information
Authors and Affiliations
About this article
Cite this article
Graffner, H., Fredlund, P., Olsson, SÅ. et al. Protective colostomy in low anterior resection of the rectum using the EEA stapling instrument. Dis Colon Rectum 26, 87–90 (1983). https://doi.org/10.1007/BF02562579
Received:
Issue Date:
DOI: https://doi.org/10.1007/BF02562579