
Abstract
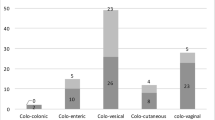
Internal fistulas in diverticular disease are uncommon and have a reputation of being difficult to treat. Eighty four patients treated from 1960 to April 1986, representing 20.4 percent (84 of 412) of the surgically treated diverticular disease patients, were reviewed. Eight patients had multiple fistulas. Sixty-five percent (60 of 92) of fistulas were colovesical, 25 percent (23 of 92) colovaginal, 6.5 percent (6 of 92) coloenteric, and 3 percent (3 of 92) colouterine fistulas. There were 66 percent (35 of 53) males and 34 percent (18 of 53) females with colovesical fistulas only. Hysterectomies had been performed in 50 percent (12 of 24) and 83 percent (19 of 23) of females with colovesical and colovaginal fistulas, respectively. Operative management included: resection anastomosis, resection with anastomosis and diversion, Hartmann procedure, and three-stage procedure. In the latter half of the series there was a significant decrease in stating procedures with no significant statistical difference in complications. There were three deaths (3.5 percent) in the series. Other complications included: wound infection, 21 percent (18 of 84), enterocutaneous fistula, 1 percent (4 of 84), and anastomotic dehiscence, 5 percent (4 of 84). Primary anastomosis can be performed with acceptable morbidity and mortality and today is the procedure of choice, leaving staging procedures to selected patients.
Similar content being viewed by others


References
Cripps WH. The passage of air and faeces per urethra. In: Cancer of the rectum: its pathology, diagnosis and treatment, including a portion of the Jacksonian prize essay for 1876. London: J&A Churchill, 1988; vii:191–206.
Couris GS, Block MA. Intestinovesical fistula. Surgery 1963;54:736–42.
Chaikof EL, Cambria RP, Warshaw AL. Colouterine fistula secondary to diverticulitis. Dis Colon Rectum 1985;28:358–60.
Colcock BP, Stahmann FD. Fistulas complicating diverticular disease of the sigmoid colon. Ann Surg 1972;175:838–46.
Mayo CW, Blunt CP. The surgical management of the complications of diverticulitis of the large intestine: analysis of 202 cases. Surg Clin North Am 1950;30:1005–12.
Bacon HE, Shindo K. Surgical management of peridiverticulitis of the colon. Surg Gynecol Obstet 1971;132:1049–51.
Pennington J, Plumb RT. Diagnosis and treatment of inflammatory vesicoenteric fistula. J Urol 1964;92:679–80.
Slade N, Gaches C. Vesico-intestinal fistulae Br J Surg 1972;59: 593–7.
Steel M, Deveney C, Burchell M. Diagnosis and management of colovesical fistulas. Dis Colon Rectum 1979;22:27–30.
Ward JN, Lavengood RW, Nay HR, Draper JW. Diagnosis and treatment of colovesical fistulas. Surg Gynecol Obstet 1970;130:1082–90.
Madden JL. Treatment of perforated lesions of the colon by primary resection and anastomosis Dis Colon Rectum 1966;9: 413–6.
Carpenter WS, Allaben RD, Kambouris A. Fistulas complicating diverticulitis of the colon. Surg Gynecol Obstet 1972;134:625–8.
Heiskell CA, Ujiki GT, Beal JM. A study of experimental colovesical fistula. Am J Surg 1975;129:316–8.
Lockhart-Mummery HE. Vesico-intestinal fistula [abridged]. Proc R Soc Med 1958;51:1032–6.
Riley FG, Bragdon FH. Pneumaturia in diabetes mellitus: report of a case. JAMA 1937;108:1596–99.
Kelly HA, MacCallum WG. Pneumaturia. JAMA 1898;31:375–81.
McSherry CK, Beal JM. Sigmoidovesical fistulae complicating diverticulitis. Arch Surg 1962;85:1024–7.
Shatila AH, Ackerman NB. Diagnosis and management of colovesical fistulas. Surg Gynecol Obstet 1976;143:71–4.
Carpenter WS, Allaben RD, Kambouris AA. One-stage resections for colovesical fistulas. J Urol 1972;108:265–7.
Rowe RJ, Sullivan ES. Fistulas of the sigmoid flexure. Dis Colon Rectum 1961;4:41–9.
Henderson MA, Small WP. Vesico-colic fistula complicating diverticular disease. Br J Urol 1969;41:314–9.
Geier GR Jr, Ujiki GT, Shields TW. Colovesical fistula. Arch Surg 1972;105:347–51.
Wychulis AR, Pratt JH. Sigmoidovaginal fistulas: a study of 37 cases. Arch Surg 1966;92:520–4.
Abcarian H, Udezue N. Coloenteric fistulas. Dis Colon Rectum 1978;21:281–6.
Hool GJ, Bokey EL, Pheils MT. Diverticular colo-enteric fistulae. Aust NZ J Surg 1981;51:358–9.
Pugh JI. On the pathology and behaviour of acquired nontraumatic vesico-intestinal fistula. Br J Surg 1964;51:644–57.
Bacon HE, Ross ST, Malvar P. Sigmoidovaginal and cecovaginal fistula as a complication of peridiverticulitis: report of eight cases. Dis Colon Rectum 1972;15:41–8.
Smalley MA, LoRusso V, O'Brien JE. Sigmoidouterine fistula complicating diverticulitis: report of a case. JAMA 1957;165: 827–8.
Rodkey GV, Welch CE. Changing patterns in the surgical treatment of diverticular disease. Ann Surg 1984;200:466–78.
Hira N. Intestinovesical fistula [summary]. Proc R Soc Med 1970; 63:243.
McGregor RA, Bacon HE. Surgical management of sigmoidovesical and sigmoido-uterine fistula complicating diverticulitis. Dis Colon Rectum 1960;3:446–8.
Best JW, Davis RM. Vesicointestinal fistulas. J Urol 1969;101:62–5.
Bacon HE, McGregor RA. Diverticular disease with particular reference to the management of concomitant fistula and sinus formation. Am J Gastroenterol 1961;36:127–32.
Author information
Authors and Affiliations
Additional information
Read at the meeting of the American Society of Colon and Rectal Surgeons, Washington, D.C., April 5 to 10, 1987.
About this article
Cite this article
Woods, R.J., Lavery, I.C., Fazio, V.W. et al. Internal fistulas in diverticular disease. Dis Colon Rectum 31, 591–596 (1988). https://doi.org/10.1007/BF02556792
Issue Date:
DOI: https://doi.org/10.1007/BF02556792