
Abstract
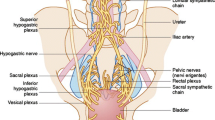
PURPOSE: Urinary dysfunction remains a common complication of radical pelvic surgery, particularly after abdominoperineal resection. In treating rectal carcinoma, the extent of primary resection and lymphadenectomy are major determinants in the degree of postoperative urologic morbidity. METHODS. Twelve male and eight female hemipelves from fresh cadavers were dissected with reference to the neuroanatomy of the lower genitourinary tract. These cadavers were dissected within twelve hours of thaw from frozen state. The cadavers were hemisected at the level of the sacral promontory for better exposure of neural trunks and vascular structures leading into the pelvis. These structures were followed down sequentially into the true pelvis, using magnified dissection under operating microscope or loupe dissection or both. RESULTS: Coordinated lower urinary tract function relies on both autonomic and somatic nerve activity. Emanating from the inferior hypogastric plexus, the pelvic nerve supplies sympathetic and parasympathetic innervation to the pelvic viscera. The course of the pelvic nerve is as follows: 1) from the inferior hypogastric plexus, it has multiple branches forming a web-like complex within the endopelvic fascial sleeve, some of which innervate the bladder detrusor; 2) a main branch traveling inferolateral to the rectum remains deep to the fascia of the levator ani muscle and courses to the external urinary sphincter; 3) at the level of the prostatic apex (or bladder neck in females), this pelvic nerve branch sends direct branches to the urinary sphincter. The pudendal nerve traverses the pelvis in the pudendal canal, and before leaving the pelvis to enter the perineum, it gives an intrapelvic branch that courses alongside the ischium to enter the external urinary sphincter. In the ischiorectal fossa, terminal branches of the pudendal nerve (i.e., perineal nerve) can be seen inserting into the urinary sphincter. CONCLUSIONS. Urinary retention and urinary incontinence represent two distinct urologic complications after abdominoperineal resection. Injury to detrusor branches of the pelvic nerve can cause detrusor denervation and urinary retention. In addition, injury to intrapelvic branches of the pelvic and pudendal nerves to the urinary sphincter can result in intrinsic sphincter deficiency and urinary incontinence. A better understanding of the neuroanatomy of the lower genitourinary tract can give a physiologic basis for clinical findings of postoperative voiding dysfunction and may help the surgeon refine surgical technique by more precisely determining resection limits to minimize urologic complications.
Similar content being viewed by others


References
Paricer SL, Tong T, Bolden S, Wingo PA. Cancer Statistics, 1997. CA Cancer J Clin, 1999;49:12.
Burgos FJ, Romero J, Fernandez E, Perales L, Tallada M. Risk factors for developing voiding dysfunction after abdominoperineal resection for adenocarcinoma of the rectum. Dis Colon Rectum 1988;31:682–5.
Kinn AC, Ohman U. Bladder and sexual function after surgery for rectal cancer. Dis Colon Rectum 1986;29:43–8.
Aagaard J, Gerstenberg TC, Knudsen JJ. Urodynamic investigation predicts bladder dysfunction at an early state after abdominoperineal resection of the rectum for cancer. Surgery 1986;99:564–8.
Rosen L, Veidenheimer MC, Coller JA, Corman ML. Mortality, morbidity, and patterns of recurrence after abdominoperineal resection for cancer of the rectum. Dis Colon Rectum 1982;25:202–8.
Gerstenberg TC, Nielson ML, Clausen S, Blaabjerg J, Lindenberg J. Bladder function after abdominoperineal resection of the rectum for anorectal surgery: urodynamic investigation before and after operation in a consecutive series. Ann Surg 1980;191:81–6.
Hojo K, Sawada T, Moriya Y. An analysis of survival and voiding, sexual function after wide iliopelvic lymphadenectomy in patients with carcinoma of the rectum, compared with conventional lymphadenectomy. Dis Colon Rectum 1989;32:128–33.
Grinnell R. Lymphatic block with atypical and retrograde lymphatic metastases and spread in carcinoma of the colon and rectum. Ann Surg 1966;163:272–80.
Cosimelli M, Mannella E, Giannarelli D,et al. Nervesparing surgery in 302 resectable rectosigmoid cancer patients: genitourinary morbidity and 10-year survival. Dis Colon Rectum 1994;37(Suppl):S42–6.
Hojo K, Vernava AM 3rd, Sugihara K, Katumata K. Preservation of urine voiding and sexual function after rectal cancer surgery. Dis Colon Rectum 1991;34:532–9.
Hollabaugh RS Jr, Dmochowski RR, Steiner MS. Neuroanatomy of the male rhabdosphincter. J Urol 1977;49:426–34.
Havenga K, Warren EE, McDermott K, Cohen AM, Minsky BD, Guillem J. Male and female sexual and urinary function after total mesorectal excision with autonomic nerve preservation for carcinoma of the rectum. J Am Coll Surg 1996;182:495–502.
Enker WE. Potency, cure, and local control in the operative treatment of rectal cancer. Arch Surg 1992;127:1396–401.
Soreide O, Norstein J. Local recurrence after operative treatment of rectal carcinoma: a strategy for change. J Am Coll Surg 1997;184:84–92.
Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal carcinoma: the clue to pelvic recurrence? Br J Surg 1982;60:613–6.
Heald RJ, Goligher JC. Anterior resection of the rectum. In: Fielding LP, Goldberg SM, eds. Surgery of the colon, rectum and anus. Rob and Smith's operative surgery. London: Chapman and Hall, 1993:456–71.
Havenga K, DeRuuiter MD, Enker WE, Welvaart K. Anatomical basis of autonomic nerve-preserving total mesorectal excision for rectal cancer. Br J Surg 1996;83:384–8.
Pavlakis AJ. Cauda equina and pelvic plexus injury. In: Krane RJ, Sirolcy MB, eds. Clinical Neuro-Urology. 2nd ed. Boston: Little, Brown, 1991:333–44.
Walsh PC, Donker PJ. Impotence following radical prostatectomy: insight into etiology and prevention. J Urol 1982;128:492–7.
Bors E. Effect of electrical stimulation of the pudendal nerves on the vesical neck; its significance for the function of cord bladders: a preliminary report. J Urol 1952;67:925–35.
Power RM. An anatomical contribution to the problem of continence and incontinence in the female. Am J Obstet Gynecol 1950;67:302–14.
Hutch JA, Rambo ON. A new theory of the anatomy of the internal urinary sphincter and the physiology of micturition. 3. Anatomy of the urethra. J Urol 1967;97:696–704.
Albert NE, Sparks FC, McGuire EJ. Effect of pelvic and retroperitoneal surgery on the urethral pressure profile and perineal floor electromyogram in dogs. Invest Urol 1977;15:140–2.
Yalla SV, Andriole GL. Vesicourethral dysfunction following pelvic visceral ablative surgery. J Urol 1984;132:503–9.
Blaivas JG, Barbalias GA. Characteristics of neural injury after abdominoperineal resection. J Urol 1983;129:84–7.
Kuru M. Nervous control of micturition. Physiol Rev 1965;45:425–94.
Author information
Authors and Affiliations
About this article
Cite this article
Hollabaugh, R.S., Steiner, M.S., Sellers, K.D. et al. Neuroanatomy of the pelvis. Dis Colon Rectum 43, 1390–1397 (2000). https://doi.org/10.1007/BF02236635
Issue Date:
DOI: https://doi.org/10.1007/BF02236635