
Abstract
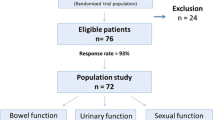
PURPOSE: Close rectal dissection is a surgical technique used by some surgeons in inflammatory bowel disease. It is performed within the mesorectum, close to the rectal muscle wall, with the aim of minimizing damage to the pelvic sexual nerves. Other surgeons dissect in the more anatomical mesorectal plane. Our aim was to determine whether close rectal dissection is more protective of the pelvic sexual nerves than mesorectal dissection. METHOD: Patients undergoing surgery for inflammatory bowel disease were entered prospectively into a database. Male patients were mailed a standardized, validated, urologic impotence questionnaire: the International Index of Erectile Function. RESULTS: There was an 81 percent response rate. Six of 156 assessable patients were totally impotent (3.8 percent). They were all in the 50-year-old to 70-year-old age group, with no impotence in patients younger than 50 years old. Twenty-one patients complained of minor diminution of erectile function (13.5 percent), where sexual activity was still possible. There was no statistical difference in the rate of complete (2.2 percentvs. 4.5 percent,P=0.67) or partial (13.5 percentvs. 13.3 percent,P=0.99) impotence between close rectal and mesorectal dissection (Fisher's exact test). There were no ejaculatory difficulties. The time elapsed since surgery ranged from 2.7 months to 192.7 months, with a median of 74.5 months. CONCLUSION: Rectal excision for inflammatory bowel disease can be conducted with low rates of impotence. Minor degrees of erectile dysfunction may be more common than currently recognized. We could not demonstrate that close rectal dissection significantly protects the patient from impotence compared with operating in the anatomical mesorectal plane. Age appears to be the most important risk factor for postoperative impotence.
Similar content being viewed by others


References
Lee EC, Dowling BL. Perimuscular excision of the rectum for Crohn's disease and ulcerative colitis. A conservative technique. Br J Surg 1972;59:29–32.
Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The International Index of Erectile Function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology 1997;49:822–30.
Lyttle JA, Parks AG. Intersphincteric excision of the rectum. Br J Surg 1977;64:413–6.
Burnham WR, Lennard-Jones JE, Brooke BN. Sexual problems among married ileostomists. Gut 1977;18:673–7.
Fazio VW, Fletcher J, Montague D. Prospective study of the effect of resection of the rectum on male sexual function. World J Surg 1980;4:149–52.
Yeager ES, Van Heerden JA. Sexual dysfunction following proctocolectomy and abdominoperineal resection. Ann Surg 1980;191:169–70.
Corman ML, Veidenheimer MC, Coller JA. Impotence after proctectomy for inflammatory disease of the bowel. Dis Colon Rectum 1978;21:418–9.
Watts J McK, de Dombal FT, Goligher JC. Long-term complications and prognosis following major surgery for ulcerative colitis. Br J Surg 1966;53:1014–23.
Donovan MJ, O'Hara ET. Sexual function following surgery for ulcerative colitis. N Engl J Med 1960;262:719–20.
Stahlgren LH, Ferguson LK. Influence on sexual function of abdominoperineal resection for ulcerative colitis. N Engl J Med 1958;259:873–5.
Prohaska JV, Siderius NJ. The surgical rehabilitation of patients with chronic ulcerative colitis. Am J Surg 1962;103:42–6.
Bauer JJ, Gelernt IM, Salky B, Kreel I. Sexual dysfunction following proctocolectomy for benign disease of the colon and rectum. Ann Surg 1983;197:363–7.
Turnbull RB. Discussion. Arch Surg 1956;73:651.
Bacon HE, Bralow SP, Berkley JL. Rehabilitation and long-term survival after colectomy for ulcerative colitis. JAMA 1960;172:324–8.
May RE. Sexual dysfunction following rectal excision for ulcerative colitis. Br J Surg 1966;53:29–30.
Leicester RJ, Ritchie JK, Wadsworth J, Thomson JP, Hawley PR. Sexual function and perineal wound healing after intersphincteric excision of the rectum for inflammatory bowel disease. Dis Colon Rectum 1984;27:244–8.
Meagher AP, Farouk R, Dozois RR, Kelly KA, Pemberton JH. J ileal pouch-anal anastomosis for chronic ulcerative colitis: complications and long-term outcome in 1310 patients. Br J Surg 1998;85:800–3.
Fazio VW, Ziv Y, Church JM,et al. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg 1995;222:120–7.
Marcello PW, Roberts PL, Schoetz DJ, Coller JA, Murray JJ, Veidenheimer MC. Long-term results of the ileoanal pouch procedure. Arch Surg 1993;128:500–3.
Becker JM, Raymond JL. Ileal pouch-anal anastomosis: a single surgeon's experience with 100 consecutive cases. Ann Surg 1986;204:375–81.
Damgaard B, Wettergren A, Kirkegaard P. Social and sexual function following ileal pouch-anal anastomosis. Dis Colon Rectum 1995;38:286–9.
Oresland T, Fasth S, Nordgren S, Hultén L. The clinical and functional outcome after restorative proctocolectomy: a prospective study in 100 patients. Int J Colorectal Dis 1989;4:50–6.
Pescatori M, Mattana C, Castagneto M. Clinical and functional results after restorative proctocolectomy. Br J Surg 1988;75:312–4.
Poppen B, Svenberg T, Bark T,et al. Colectomy-proctomucosectomy with S-pouch: operative procedures, complications and functional outcome in 69 consecutive patients. Dis Colon Rectum 1992;35:40–7.
Tiainen J, Matikainen M, Hiltunen K-M. Ileal J-pouchanal anastomosis, sexual dysfunction and fertility. Scand J Gastroenterol 1999;34:185–8.
Michalessi F, Stella M, Block GE. Prospective assessment of functional results after ileal J pouch-anal restorative proctocolectomy. Arch Surg 1993;128:889–95.
Keighley MR, Grobler S, Bain I. An audit of restorative proctocolectomy. Gut 1993;34:680–4.
Setti-Carraro P, Ritchie JK, Wilkinson KH, Nicholls RJ, Hawley PR. The first 10 years' experience of restorative proctocolectomy for ulcerative colitis. Gut 1994;35:1070–5.
Emblem R, Bergan A, Flatmark A. Mucosal proctectomy with straight ileoanal anastomosis. Scand J Gastroenterol 1988;23:1165–72.
Skarsgard ED, Atkinson KG, Bell GA, Pezim ME, Seal AM, Sharp FR. Function and quality of life results after ileal pouch surgery for chronic ulcerative colitis and familial polyposis. Am J Surg 1989;157:467–71.
Wexner SD, Jensen L, Rothenberger DA, Wong WD, Goldberg SM. Long-term functional analysis of the ileoanal reservoir. Dis Colon Rectum 1989;32:275–81.
Finkle AL, Moyers TG, Tobenkin MI, Karg SJ. Sexual potency in aging males. JAMA 1959;170:1391–3.
Pearlman CK, Kobashi LI. Frequency of intercourse in men. J Urol 1972;107:298–301.
Author information
Authors and Affiliations
Additional information
Read at the Royal Society of Medicine, Section of Coloproctology, Short Papers Meeting, London, United Kingdom, November 24, 1999.
Dr. Ian Lindsey is supported by the Colorectal Research Fund.
About this article
Cite this article
Lindsey, I., George, B.D., Kettlewell, M.G.W. et al. Impotence after mesorectal and close rectal dissection for inflammatory bowel disease. Dis Colon Rectum 44, 831–835 (2001). https://doi.org/10.1007/BF02234703
Issue Date:
DOI: https://doi.org/10.1007/BF02234703