
Summary
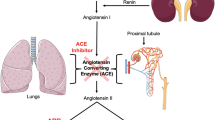
Angiotensin converting enzyme (ACE) inhibitors are a novel class of antihypertensive and anticongestive heart failure agents with wide patient and physician acceptability. By blocking the formation of angiotensin II in blood and tissues, all ACE inhibitors significantly lower systemic vascular resistance, lower blood pressure, and improve cardiac function, while maintaining or enhancing perfusion of vital organs: kidneys, brain, and heart. Captopril is the first oral ACE inhibitor with an active sulfhydryl group. Enalapril and lisinopril are potent nonsulfhydryl inhibitors of ACE characterized by weak chelating properties. The side effects of skin rashes, pruritis, taste abnormalities, oral ulcers, pemphigus, and blood dyscrasias have been considered to be strongly characteristic of penicillaminelike drugs, including the sulfhydryl ACE inhibitors. The class effects of cough, angioedema, hyperkalemia, nonoliguric functional renal insufficiency, and hypotension can occur with equal frequency with all ACE inhibitors. It is unclear whether the many yet investigational ACE inhibitors would have distinct advantages over captopril, enalapril, lisinopril, and enalaprilat. This paper reviews the comparative structure and clinical pharmacology of the three commercially available but chemically different oral ACE inhibitors.
Similar content being viewed by others


References
Goldblatt HJ, Lynch RF, Hanzal RF, et al. Studies on experimental hypertension: Production of persistent elevation of systolic blood pressure by means of renal ischemia.J Exp Med 1934;49:347–379.
Ondetti MA, Williams NJ, Sabo EF, et al. Angiotensin converting enzyme inhibitors from the venom ofBathrops jararaca: Isolation, elucidation of structure and synthesis.Biochemistry 1971;10:4033–4039.
Ondetti MA, Rubin B, Cushman DW. Design of specific inhibitors of angiotensin converting enzyme: New class of orally active antihypertensive agents.Science 1977;196:441–444.
Cushman DW, Cheung HS, Sabo EF, et al. Design of potent competitive inhibitors of angiotensin converting enzyme: Carboxyalkanoyl and mercaptoalkanoyl amino acids.Biochemistry 1977;16:548–591.
Patchett AA, Harris E, Tristran EW, et al. A new class of angiotensin-converting enzyme inhibitors.Nature 1980;288: 280–283.
Skeggs LT, Kahn JR, Shumway NP. The preparation and function of the hypertension converting enzyme.J Exp Med 1956;103:295–299.
Wyvrat MJ, Patchett AA. Recent developments in the design of angiotensin-converting enzyme inhibitors.Med Res Rev 1985;5:483–531.
Petrillo EW, Powell JR, Cushman DW, et al. Angiotensin converting enzyme inhibitors: Accomplishments and challenges.Clin Exp Hypertens 1987;A9(283):235–241.
Karanewsky DS, Badia MC, Cushman DW, et al. Novel orally active inhibitors of angiotensin-converting enzyme.Proc 192nd ACS Natl Meeting 1986, Abst Medi 8.
Kostis JB. Angiotensin-converting enzyme inhibitors: Emerging differences and new compounds.Am J Hypertens 1989;2:57–64.
Dzau VJ. Circulating versus local renin-angiotensin system in cardiovascular homeostasis.Circulation 1988;77 (Suppl I):14–113.
Campbell DJ. Circulating and tissue angiotensin systems.J Clin Invest 1987;79:1–6.
Wilson SK, Lynch DR, Snyder SH. Angiotensin-converting enzyme labeled with [3H] captopril.J Clin Invest 1987; 80:841–850.
McGiff JC, Terragno NA, Malik KU, et al. Release of prostaglandin E-like substance from canine kidney by bradykinin.Circ Res 1972;31:36–43.
Brogden RN, Todd PA, Sorkin EM. Captopril, an, update of its pharmacodynamic and pharmacokinetic properties and therapeutic use in hypertension and congestive heart failure.Drugs 1988;36:540–600.
Swartz SL, Williams GH. Angiotensin-converting enzyme inhibition and prostaglandins.Am J Cardiol 1982;49:1405–1409.
Mookherjee S, Anderson GH, Eich R, et al. Acute effects of captopril on cardiopulmonary hemodynamics and reninangiotensin-aldosterone and bradykinin profile in hypertension.Am Heart J 1983;105:106–112.
Nishimura H, Kubo S, Ueyama M, et al. Effects of captopril on peripheral hemodynamics in severe congestive heart failure.Clin Exp Hypertens 1987;A9:587–591.
Salvetti A, Pedrinelli R, Magagna A, et al. Differential effects of selective and non-selective prostaglandin-synthesis inhibition on the pharmacological responses to captopril patients with essential hypertension.Clin Science 1982; 63:261S–263S.
Sweet CS, Gaul SL, Reitz AM, et al. Mechanism of action of enalapril in experimental hypertension and acute left ventricular failure.J Hypertens 1983;1 (Suppl 1):53–63.
Oparil S, Horton R, Wilkins LH, et al. Antihypertensive effect of enalapril (MK-421) in low renin essential hypertension: Role of Vasodilator prostaglandins. (abstract).Clin Res 1983;31:538A.
Todd PA, Heel RC. Enalapril, a review of its pharmacodynamic and pharmacokinetic properties and therapeutic use in hypertension and congestive heart failure.Drugs 1986; 31:198–248.
Singhvi SM, McKinstry DN, Shaw JM, et al. Effect of food on the bioavailability of captopril in healthy subjects.J Clin Pharmacol 1982;22:135–140.
Swansons BN, Vlasses PH, Ferguson RK, et al. Influence of food on the bioavailability of enalapril.J Pharm, Sci 1984; 73:1655–1657.
Hommel E, Hans-Henrik P, Mathiesen E, et al. Effect of captopril on kidney function in insulin-dependent diabetic patients with nephropathy.Br Med J 1986;293:467–470.
Marre M, Leblanc H, Suarez L, et al. Converting enzyme inhibition and kidney function in normotensive diabetic patients with persistent microalbuminuria.Br Med J 1987; 294:1448–1452.
Lancester SG, Todd PA. Lisinopril, a preliminary review of its pharmacodynamic and pharmacokinetic properties and therapeutic use in hypertension and congestive heart failure.Drugs 1988;35:646–669.
Migdalof BH, Antonaccio MJ, McKinstry DN, et al. Captopril: Pharmacology, metabolism and disposition.Drug Metab Rev 1984;15:841–869.
Westlin W, Mullane K. Does captopril attenuate reperfusion-induced myocardial dysfunction by scavenging free radicals?Circulation 1988;77 (Suppl 1):130–139.
Gomez HJ, Cieillo VJ, Davis RO, et al. Enalapril in congestive heart failure: Acute and chronic invasive hemodynamic evaluation.Int J Cardiol 1986;11:37–48.
Blythe WB. Captopril and renal autoregulation.N Engl J Med 1983;308:390–391.
Thind GS. Renal insufficiency during angiotensin-converting enzyme inhibitor therapy in hypertensive patients with no renal artery stenosis.J Clin Hypertens 1985;4:337–343.
Bauer JH, Reams GP, Lal SM. Renal protective effect of strict blood pressure control with enalapril therapy.Arch Intern Med 1987;147:1397–1400.
Anderson S, Meyer TW, Renke HG, et al. Control of glomerular hypertension limits glomerular injury in rats with reduced renal mass.J Clin Invest 1985;76:612–619.
Zatz R, Dunn BR, Meyer TW, et al. Prevention of diabetic glomerularopathy by pharmacological amelioration of glomerular capillary hypertension.J Clin Invest 1986;77:1925–1930.
Anderson S, Brenner BM. Effects of aging on the renal glomerulus.Am J Med 1986;80:435–442.
Raij L, Chiou X, Owens R, et al. Therapeutic implications of hypertension-induced glomerular injury.Am J Med 1985; 79:37–41.
Bauer JH, Jones LB. Comparative studies: Enalapril versus hydrochlorothiazide a first-step therapy for the treatment of primary hypertension.Am J Kidney Dis 1984;4:55–62.
Vetter W, Wehling M, Foerster ECh, et al. Long-term effect of captopril on kidney function in various forms of hypertension.Klin Wochenschr 1984;62:731–737.
De Venuto G, Andreotti C, Mattarei M, et al. Prolonged treatment of essential hypertension and renal function: Comparison of captopril and beta-blockers considering microproteinuria values.Curr Ther Res 1985;38:710–718.
Ondetti MA. Structure relationship of angiotensin converting enzyme inhibitors ot pharmacologic activity.Circulation 1988;77 (Suppl I):174–178.
Zussman RM. Renin and nonrenin mediated antihypertensive action of converting enzyme inhibitors.Kidney Int 1984;25:969–983.
Jaffe IA. Adverse effects profile of sulfhydryl compounds in man.Am J Med 1986;80:471–476.
Thind GS. Demography predicts blood pressure response to once-daily enalapril monotherapy of mild-to-moderate essential hypertensive patients.Am J Hypertens 1988;1:227S–229S.
Thind GS. Lisinopril versus atenolol alone and with hydrochlorothiazide in the treatment of mild-to-moderate essential hypertension.J Hypertens 1986;4 (Suppl 5):S423–S425.
Thind GS, Johnson A, Bhatnagar D, et al. A parallel study of enalapril and captopril and 1 year of experience with enalapril treatment in moderate-to-severe essential hypertension.Am Heart J 1985;109:852–858.
Thind GS, Mahapatra RK, Johnson A, et al. Low-dose captopril titration in patients with moderate-to-severe hypertension treated with diuretics.Circulation 1983;67:1340–1346.
The Concensus Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure.N Engl J Med 1987;316:1429–1435.
Todd PA, Goa KL. Enalapril: An update on its pharmacological properties and therapuetic use in congestive heart failure.Drugs 1989;37:141–161.
Packer M, Lee WH, Yashak M, et al. Comparison of captopril and enalapril in patients with severe chronic heart failure.N Engl J Med 1986;315:847–853.
Abramowicz M (ed). ACE inhibitors for congestive heart failure.Med Lett 1988;30:97–98.
Rutledge J, Ayers C, Davidson R, et al. Effect of intravenous enalaprilat in moderate and severe systemic hypertension.Am J Cardiol 1988;62:1062–1067.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Thind, G.S. Angiotensin converting enzyme inhibitors: Comparative structure, pharmacokinetics, and pharmacodynamics. Cardiovasc Drug Ther 4, 199–206 (1990). https://doi.org/10.1007/BF01857634
Issue Date:
DOI: https://doi.org/10.1007/BF01857634