
Abstract
We repeatedly assessed pulmonary and systemic haemodynamics in 40 adult patients undergoing therapy for severe acute respiratory failure of diverse causes (ARDS). Initial measurements were performed just before admission to our Intensive Care Unit (first haemodynamic evaluation) and were repeated during the course of illness, after correcting hypoxemia, hypercapnia and acidosis by mechanical ventilation with high FiO2 and positive end expiratory pressure, or by extracorporeal membrane oxygenation. In some patients pulmonary blood flow (PBF) was increased by dopamine infusion or reduced by partial veno arterial bypass.
First haemodynamic evaluation permitted us to individualize four systemic haemodynamic patterns in the early stage of ARDS; hyperkinetic state (17 cases), hypovolemia (12 cases), myocardial failure (4 cases) or over-perfusion (6 cases).
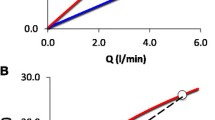
Our measurements pointed out that pulmonary hypertension is a usual finding in ARDS (mean pulmonary artery pressure: 26±7 mmHg for PBF=1−2 1/min/sq.meter); 25±6 mmHg for PBF=2−3 1/min/sq.meter; 26±7 mmHg for PBF=3−4 1/min/sq.meter) with a high pulmonary vascular resistance (PVR=14±3 mmHg/1 for PBF=1−2 1/min/sq.meter; 8±3 mmHg/1 for pBF=2−3 1/min/sq.meter; 5±2 mmHg/1 for PBF=3−4 1/min/sq.meter); we found also that pulmonary hypertension and pulmonary vascular resistance increased progressivly in patients who died.
Pulmonary hypertension in ARDS has two haemodynamic consequences:
1° It causes an elevated afterload for the right ventricle with an excessive right ventricular stroke-work index wich can produce right heart failure.
2° It is probably in part responsible for an abnormally low systemic arterial pressure (47±16 mmHg for PBF=1−2 1/min/sq.meter; 54±11 mmHg for PBF=2−3 1/min./sq.meter; 64±17 mmHg for PBF=3−4 1/min/sq.meter) and a low systemic arterial resistance (24±9 mmHg/1 for PBF=1−2 1/min.sq.meter; 19±5 mmHg/1 for PBF=2−3 1/min/sq.meter; 17±5 mmHg/1 for PBF=3−4 1/min/sq.meter) observed in our patients with ARDS.
The major therapeutic goal of respiratory intensive therapy in severe acute respiratory failure (ARF) caused by altered permeability oedema (APE) is to control the arterial hypoxemia that results from a high intrapulmonary shunt. In addition to respiratory therapy, careful attention must be given to the recognition and management of systemic haemodynamic disturbances complicating the early state of A.P.E.: such disorders as a hyperkinetic state, myocardial failure, hypovolaemia or overperfusion can enhance hypoxemia and myocardial failure or hypovolaemia may be worsened by the use of mechanical ventilation with positive end-expiratory pressure (PEEP). Moreover during the course of ARF with the development of progressive pulmonary fibrosis the alteration in the pulmonary arterial tree produces a high right ventricular after-load with the risk of acute Cor pulmonale.
This study was undertaken to describe the early haemodynamic disorders coexisting with APE and to assess pulmonary and systemic haemodynamics during the course of ARF [managed with mechanical ventilation and PEEP, and in some cases with extracorporeal membrane oxygenation (ECMO)].
Similar content being viewed by others


References
Lemaire, F., Jardin, F., Harari, A., Teisseire, B., Laurent, D., Rapin, M.: Assessment of gas exchange during veno arterial bypass using the membrane lung. In: Artificial lung for acute respiratory failure. Zapol, W., Quist, J. (eds.), pp 421–433 New York: Academic Press 1976
Lemaire, F., Jardin, F., Regnier, B., Loisance, D., Goudot, B., Lange, F., Eveleigh, M.C., Teisseire, B., Laurent, D., Rapin, M.: Pulmonary gas exchange during veno arterial bypass with a membrane lung for acute respiratory failure. J. Thorac. Cardiovac. Surg. 6, 839–846 (1978)
Barrat-Boyes, B.G., Wood, E.H.: Cardiac output and related measurements and pressure values in the right heart and associated vessels, together with an analysis of the haemodynamic response to the inhalation of high oxygen mixtures in healthy subjects. J. Lab. Clin. Med.51, 72–90 (1958)
Holmgren, A., Jonsson, B., Stöstrand, T.: Circulatory data in normal subjects at rest and during exercise in recumbent position, with special reference to the stroke volume at different work intensities. Acta Physiol. Scand.49, 343–363 (1960)
Pemberton, L.B.: Shock lung with massive tracheal loss of plasma. JAMA273 (23), 2511–2513 (1977)
Weil, M.H., Henning, R.J.: Acute circulatory failure (shock) associated with cardiogenic pulmonary edema. Crit. Care Med.5, 215–219 (1977)
Tenaillon, A., Labrousse, J., Merillon, J.P., Guiomard, A., Bousser, J.P., Lissac, J.: Hypovolemia after acute pulmonary edema. Intens. Care Med.3, 107 (1977)
Figueras, J., Weil, M.H.: Blood volume prior to and following treatment of acute cardiogenic pulmonary edema. Circulation57, 349–354 (1978)
Lemaire, F., Teisseire, B., Harari, A., Loisance, D.: La PaO2 en oxygène pur est elle un critère fiable du transfert pulmonaire d'oxygène au cours des assistances respiratoires par poumon à membrane. Nouv. Press. Méd.3, 1815 (1974)
Darragon, T., Dussan, J., Estopa, R., Regnier, B., Lemaire, F., Rapin, M., Teisseire, B.: Syndrome hémodynamique hyperkinétique au cours des pneumopathies fulminantes. Nouv. Press. Méd.6, 3118 (1977)
Jardin, F., Delille, F., Gurdjian, F., Blanchet, F., Margairaz, A.: Profil hémodynamique du syndrome de détresse respiratoire aiguë de l'adulte. Nouv. Press. Méd.6, 3401–3406 (1977).
Jardin, F., Gurdjian, F., Eveleight, M.C., Fouilladieu, J.L., Margairaz, A.: Immediate and middle term cardiorespiratory effects of positive end-expiratory pressure in thirten cases of non-haemodynamic pulmonary edema. Rescuscitation6, 125–129 (1978)
Zapol, W.H., Snider, M.T.: Pulmonary hypertension in severe acute respiratory failure. New Engl. J. Med. 296, 476–480 (1977)
Eklund, L.G., Holmgren, A.: Central hemodynamics during exercice. Circul. Res.20 and22 (Suppl. 1), 33–43 (1967)
Widmsky, J., Riedel, M., Stanek, V.: Central hemodynamics during exercise in patients with restrictive pulmonary disease. Bull. Eur. Physiopathol. Respir.13, 369–379 (1977)
Zapol, N.M., Kobayashi, K., Snider, M.P., Greene, R., Laver, M.B.: Vascular obstruction causes pulmonary hypertension in severe acute respiratory failure. Chest71, 306–307 (1977)
Laks, M.M., Garder, D., Morad, F., Swan, H.J.C.: Hemodynamics in the consious dog during progressive pulmonary arterial occlusion. Am. J. Physiol.222, 578–582 (1972)
Thal, A.P.: Shock: A physiologic basis for treatment, pp. 210–215. Chicago: Year Book Medical Publishers Inc. 1971
Clowes, G.M.A., O'Donnel, T.F., Ryan, N.T., Blackburn, G.L.: Energy metabolism in sepsis: treatment based on different patterns in shock and high output stage. Ann. Surg. 684–696 (1974)
Winslow, E.J., Loeb, H.J., Rahimtoola, S.H., Kamath, S., Gunnar, R.M.: Hemodynamic studies and results of therapy in 50 patients with bacteremic shock. Am. J. Med.54, 421–432 (1973)
Ashbaugh, D.G., Petty, T.L.: Sepsis complicating the acute respiratory distress syndrome. Surgery gynecology and obstetrics6, 865–869 (1972)
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Jardin, F., Gurdjian, F., Fouilladieu, J.L. et al. Pulmonary and systemic haemodynamic disorders in the adult respiratory distress syndrome. Intensive Care Med 5, 127–133 (1979). https://doi.org/10.1007/BF01683194
Issue Date:
DOI: https://doi.org/10.1007/BF01683194