
Abstract
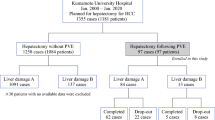
We retrospectively classified patients with hepatocellular carcinoma by the results of tests of 15-minute indocyanine green retention (ICGR15). Of the 201 patients with hepatocellular carcinoma admitted to our department in the past 6 years, 36 patients were assigned to group 1 (ICGR15 <10.0%), 81 patients to group 2 (ICGR15=10.1–20.0%), and 84 patients to group 3 (ICGR15≥20.1%). Of the total 201 patients, 72% underwent liver resection (78% of group 1 patients, 80% of group 2 patients, and 62% of group 3 patients).
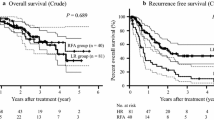
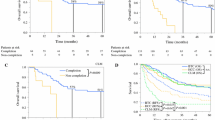
We regarded the cirrhosis of the patients in group 3 as severe and studied their survival rate classified by the treatment used. Of these 84 patients, 52 patients were treated by liver resection, about half of whom were treated preoperatively by transcatheter arterial embolization (TAE). Another 9 patients were treated preoperatively by both TAE and portal vein embolization (PVE). At 2 years, and again at 3 years, the survival rate was significantly higher when TAE was used preoperatively than with resection alone. We think that the possibility of performing needed liver resection will be enlarged by preoperative PVE and that liver resection can be done more safely after use of PVE in some patients.
Résumé
Nous avons classé rétrospectivement des patients présentant un cancer hépatocellulaire selon les résultats d'un test de rétention pendant 15 minutes du vert indocyanique (RVIC15). Au cours des 6 dernières années, sur 201 patients admis dans notre département et présentant un cancer hepatocellulaire, 36 appartenaient au groupe 1 (RVIC15<10.0%), 81 au groupe 2 (RVIC=10.1–20.0%), et 84 au groupe 3 (RVIC15≥20.1%). Sur 201 patients, 72% ont subi une résection hépatique (78% dans le groupe 1, 80% dans le groupe 2, et 62% dans le groupe 3). Dans le groupe 3, la cirrhose était considérée comme grave. Nous avons ensuite étudié la survie selon le type de traitement. Parmi les 84 patients du groupe 3, 52 ont subi une résection hépatique. La moitié d'entre eux a subi en période préopératoire une embolisation artérielle par cathéter (EAC). Neuf patients ont eu une EAC et une embolisation de la veine porte (EVP). La survie à 2 et 3 ans était plus longue de façon significative lorsque les patients avaient eu une EAC avant l'opération par rapport à ceux qui n'avaient eu qu'une résection. Nous pensons que les indications de la résection hépatique peuvent être élargies grâce à la EAC préopératoire et que l'EAC augmente la sécurité de la chirurgie hépatique dans certains cas.
Resumen
Hemos clasificado retrospectivamente a los pacientes con carcinoma hepatocelular mediante los resultados de la prueba de retención a 15 minutes del verde indociamina (VIC15). De los 201 pacientes con carcinoma hepatocellular ingresados a nuestro departamento en los últimos 6 años, 36 fueron asignados al grupo 1 (VIC15<10.0%), 81 al grupo 2 (VIC15=10.1–20.0%), y 84 al grupo 3 (VIC15≥20.1%). Del total de los 201 pacientes, 72% fueron sometidos a resección hepática: 78% del grupo 1, 80% del grupo 2, y 62% del grupo 3.
Consideramos como severa la cirrosis de los pacientes en el grupo 3 y analizamos su tasa de supervivencia de acuerdo a la modalidad de tratamiento utilizado. De estos 84 pacientes, 52 fueron sometidos a resección hepática y en alrededor de la mitad se realizó embolización preoperatoria por catéter transarterial (ECTA). Otros 9 fueron tratados preoperatoriamente mediante ECTA y embolización por vía de la vena porta (EVP). A los 2 años, y también a los 3 años, la tasa de supervivencia fue significativamente mayor cuando se realizó ECTA preoperatoriamente que cuando se realizó solamente la resección. Creemos que la posibilidad de realizar la necesaria resección hepática puede ser ampliada mediante la EVP y que la resección puede ser lograda en forma más segura después de la EVP en algunos casos.
Similar content being viewed by others
References
Liver Cancer Study Group of Japan: Survey and follow-up study of primary liver cancer in Japan. The 7th report (in Japanese). Kanzo27:1164, 1986
Liver Cancer Study Group of Japan: The General Rules for the Clinical and Pathological Study of Primary Liver Cancer, 2nd edition (in Japanese), Tokyo, Kanehara-Syuppan, 1987, pp. 24–25
Yamada, R., Sato, M., Kawabata, H., Nakatsuka, H., Nakamura, K., Takashima, S.: Artery embolization in 120 patients with unresectable hepatoma. Radiology148:397, 1983
Kinoshita, H., Sakai, K., Hirohashi, K., Igawa, S., Yamazaki, O., Kubo, S.: Preoperative portal vein embolization for hepatocellular carcinoma. World J. Surg.10:803, 1986
Iwatsuki, S., Shaw, B.W., Starzl, T.E.: Experience with 150 liver resections. Ann. Surg.197:247, 1983
Balasegaram, M., Joishy, S.K.: Hepatic resection: Pillars of success built on the foundation of 15 years of experience. Am. J. Surg.141:360, 1981
Tao, Q.-M., Yoeh, E.-K., Tandon, B.N., Noer, H.M.S., Sulaiman, H.A., Akbar, N., Lesmana, L.A., Hirayama, T., Chung, W.-K., Shrestha, S.M., Chan, S.-H., Viranuvatti, V.: Epidemiology of hepatocellular carcinoma. In Hepatocellular Carcinoma in Asia, Kobe, International Center for Medical Research, Kobe University School of Medicine, 1985, pp. 3–66
Okamoto, E., Tanaka, N., Yamanaka, N., Toyosaka, A.: Results of surgical treatments of primary hepatocellular carcinoma: Some aspects to improve long-term survival. World J. Surg.8:360, 1984
Goldstein, H.M., Wallace, S., Anderson, J.H., Bree, R.L., Gianturco, C.: Transcatheter occlusion of abdominal tumors. Radiology120:539, 1976
Okudaira, M., Sasaki, K., Naka, H.: Vascular architecture of malignant neoplasms (in Japanese). Myakkangaku19:229, 1979
Hirohashi, K., Sakaj, K., Kinoshita, H., Igawa, S., Matsuoka, S., Nagata, E., Kubo, S.: Hepatectomy after transcatheter arterial embolization (TAE) for hepatocellular carcinomas (in Japanese). Nippon Geka Gakkai Zasshi86:555, 1985
Nakashima, T.: Pathology of hepatocellular carcinoma: Tumor thrombus of the portal vein (in Japanese). Kanzo25:120, 1984
Herrmann, R.E.: Medical and surgical problems of portal hypertension patients selection and classes of risk. In Medical and Surgical Problems of Portal Hypertension, M.J. Orloff, S. Stipa, V. Ziparo, editors, New York, Academic Press, 1980, p. 93
Takeshige, K., Yamamoto, S., Kojima, H., Arakawa, T., Kuroda, H., Kawai, Y., Fukuya, Y.: An analysis of prognostic examination in cirrhotic portal hypertension and hepatoma (in Japanese). Nippon Geka Gakkai Zasshi87:206, 1986
Ozawa, K., Ida, T., Yamada, T., Honjo, K.: Significance of glucose tolerance as prognostic sign in hepatectomized patients. Am. J. Surg.131:541, 1976
Tsukada, K.: Clinical study on hepatic extraction rate of ICG in patients with portal hypertension (in Japanese). Kanzo27:1313, 1986
Takahashi, K., Saito, M., Tanaka, H., Asaka, M., Nagase, K., Miyazaki, T.: Significance of ICG test for prognosis of liver diseases (in Japanese). Jpn. Pharmacol. Therapeutics10[Suppl. 1]:157, 1982
Author information
Authors and Affiliations
Additional information
Supported in part by a Grant-in-Aid for Cancer Research (59-6) from the Ministry of Health and Welfare.
Rights and permissions
About this article
Cite this article
Fujio, N., Sakai, K., Kinoshita, H. et al. Results of treatment of patients with hepatocellular carcinoma with severe cirrhosis of the liver. World J. Surg. 13, 211–217 (1989). https://doi.org/10.1007/BF01658403
Issue Date:
DOI: https://doi.org/10.1007/BF01658403