
Abstract
Background
The optimal extent of therapeutic lateral neck dissection (ND) in papillary thyroid carcinoma (PTC) continues to be debated. We analyzed the frequency, patterns, and predictive factors of occult level Va and Vb metastasis in clinically lateral node-positive PTC patients.
Methods
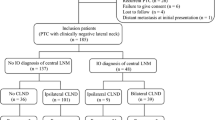
We reviewed the data of PTC patients who underwent thyroidectomy and therapeutic lateral ND from level II to V between May 2008 and August 2020. In our study, 46 patients without clinically positive metastatic lymph nodes (LNs) at level V on the preoperative evaluation were included to analyze occult metastasis at level Va and Vb, respectively. Patient demographics, including age, sex, distribution of pathologic LNs, and characteristics of the primary tumors, were reviewed. In addition, clinicopathologic factors associated with occult level Va and Vb metastasis were analyzed.
Results
Of the 46 patients, 14 (30.4%) patients had occult metastases at level Vb. No occult metastases were found at level Va. Clinically positive level II metastasis (p = 0.015) and simultaneous level II, III, and IV metastases (p = 0.010) in the preoperative evaluation were significantly associated with occult level Vb metastasis. Patients without LN metastasis at level IV or with three or fewer metastatic LNs in the lateral neck never had occult LN metastases at level Vb.
Conclusions
Occult metastasis at level Va is rare in PTC with lateral LN metastasis. Occult metastasis at level Vb may occur in PTC patients with multilevel involvement, including level II and/or four or more lateral LN metastases.
Similar content being viewed by others


References
Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. 1994;97:418–28.
Shaha AR. Prognostic factors in papillary thyroid carcinoma and implications of large nodal metastasis. Surgery. 2004;135:237–9.
Ahn SH. Usage and diagnostic yield of fine-needle aspiration cytology and core needle biopsy in thyroid nodules: a systematic review and meta-analysis of literature published by Korean authors. Clin Exp Otorhinolaryngol. 2021;14:116–30.
Wang TS, Dubner S, Sznyter LA, Heller KS. Incidence of metastatic well-differentiated thyroid cancer in cervical lymph nodes. Arch Otolaryngol Head Neck Surg. 2004;130:110–3.
Lin DZ, Qu N, Shi RL, Lu ZW, Ji QH, Wu WL. Risk prediction and clinical model building for lymph node metastasis in papillary thyroid microcarcinoma. Oncol Targets Ther. 2016;9:5307–16.
Kim SK, Park I, Woo JW, Lee JH, Choe JH, Kim JH, et al. Predictive factors for lymph node metastasis in papillary thyroid microcarcinoma. Ann Surg Oncol. 2016;23:2866–73.
Machens A, Hinze R, Thomusch O, Dralle H. Pattern of nodal metastasis for primary and reoperative thyroid cancer. World J Surg. 2002;26:22–8.
Bhattacharyya N. Surgical treatment of cervical nodal metastases in patients with papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2003;129:1101–4.
Ahn SH, Kim WS. The effect of prophylactic central neck dissection during hemithyroidectomy on locoregional recurrence in patients with papillary thyroid carcinoma: a meta-analysis. Clin Exp Otorhinolaryngol. 2020;13:194–202.
Inoue H, Nibu K, Saito M, Otsuki N, Ishida H, Onitsuka T, et al. Quality of life after neck dissection. Arch Otolaryngol Head Neck Surg. 2006;132:662–6.
Terrell JE, Welsh DE, Bradford CR, Chepeha DB, Esclamado RM, Hogikyan ND, et al. Pain, quality of life, and spinal accessory nerve status after neck dissection. Laryngoscope. 2000;110:620–6.
Kim SK, Park I, Hur N, Lee JH, Choe JH, Kim JH, et al. Should level V be routinely dissected in n1b papillary thyroid carcinoma? Thyroid. 2017;27:253–60.
Won HR, Chang JW, Kang YE, Kang JY, Koo BS. Optimal extent of lateral neck dissection for well-differentiated thyroid carcinoma with metastatic lateral neck lymph nodes: a systematic review and meta-analysis. Oral Oncol. 2018;87:117–25.
Javid M, Graham E, Malinowski J, Quinn CE, Carling T, Udelsman R, et al. Dissection of levels II through v is required for optimal outcomes in patients with lateral neck lymph node metastasis from papillary thyroid carcinoma. J Am Coll Surg. 2016;222:1066–73.
Lima LP, Amar A, Lehn CN. Spinal accessory nerve neuropathy following neck dissection. Braz J Otorhinolaryngol. 2011;77:259–62.
Lee BJ, Wang SG, Lee JC, Son SM, Kim IJ, Kim YK. Level IIb lymph node metastasis in neck dissection for papillary thyroid carcinoma. Arch Otolaryngol Head Neck Surg. 2007;133:1028–30.
Koo BS, Yoon YH, Kim JM, Choi EC, Lim YC. Predictive factors of level IIb lymph node metastasis in patients with papillary thyroid carcinoma. Ann Surg Oncol. 2009;16:1344–7.
Lim YC, Choi EC, Yoon YH, Koo BS. Occult lymph node metastases in neck level V in papillary thyroid carcinoma. Surgery. 2010;147:241–5.
Yang J, Gong Y, Yan S, Zhu J, Li Z, Gong R. Risk factors for level V lymph node metastases in solitary papillary thyroid carcinoma with clinically lateral lymph node metastases. Cancer Med. 2016;5:2161–8.
Stack BC Jr, Ferris RL, Goldenberg D, Haymart M, Shaha A, Sheth S, et al. American Thyroid Association consensus review and statement regarding the anatomy, terminology, and rationale for lateral neck dissection in differentiated thyroid cancer. Thyroid. 2012;22:501–8.
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133.
Perros P, Boelaert K, Colley S, Evans C, Evans RM, Gerrard Ba G, et al. Guidelines for the management of thyroid cancer. Clin Endocrinol (Oxf). 2014;81(Suppl 1):1–122.
Kupferman ME, Patterson DM, Mandel SJ, LiVolsi V, Weber RS. Safety of modified radical neck dissection for differentiated thyroid carcinoma. Laryngoscope. 2004;114:403–6.
Kim SK, Park I, Hur N, Choe J-H, Kim J-H, Kim JS. Patterns, predictive factors and prognostic impact of multilevel metastasis in N1b papillary thyroid carcinoma. Br J Surg. 2017;104:857–67.
Roh JL, Kim JM, Park CI. Lateral cervical lymph node metastases from papillary thyroid carcinoma: pattern of nodal metastases and optimal strategy for neck dissection. Ann Surg Oncol. 2008;15:1177–82.
King JM, Corbitt C, Miller FR. Management of lateral cervical metastases in papillary thyroid cancer: patterns of lymph node distribution. Ear Nose Throat J. 2011;90:386–9.
Farrag T, Lin F, Brownlee N, Kim M, Sheth S, Tufano RP. Is routine dissection of level II-B and V-A necessary in patients with papillary thyroid cancer undergoing lateral neck dissection for FNA-confirmed metastases in other levels. World J Surg. 2009;33:1680–3.
Kupferman ME, Weinstock YE, Santillan AA, Mishra A, Roberts D, Clayman GL, et al. Predictors of level V metastasis in well-differentiated thyroid cancer. Head Neck. 2008;30:1469–74.
Sivanandan R, Soo KC. Pattern of cervical lymph node metastases from papillary carcinoma of the thyroid. Br J Surg. 2001;88:1241–4.
Zhang X-J, Liu D, Xu D-B, Mu Y-Q, Chen W-K. Should level V be included in lateral neck dissection in treating papillary thyroid carcinoma? World J Surg Oncol. 2013;11:304.
Acknowledgment
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant Number: HR20C0025), the Patient-Centered Clinical Research Coordinating Center funded by the Ministry of Health & Welfare, Republic of Korea (Grant number: HI19C0481, HC19C0103), and the National Research Foundation of Korea (NRF) (Grant Number: 2019R1A2C1084125).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors declare that there are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Song, K., Jin, Y., Kim, M. et al. Patterns of Occult Metastasis to Level Va and Vb in Clinically Lateral Node-Positive Papillary Thyroid Carcinoma. Ann Surg Oncol 29, 2550–2556 (2022). https://doi.org/10.1245/s10434-021-11085-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-11085-9