
Abstract
Background
Papillary thyroid cancer (PTC) frequently disseminates into cervical lymph nodes. Lateral node involvement is described in up to 50 % patients undergoing prophylactic lateral neck dissection. This study aimed to assess this finding and identify which factors predict for occult lateral node disease.
Methods
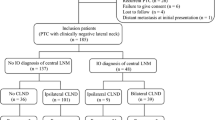
Patients with fine needle aspiration–confirmed PTC (Bethesda V or VI), without evidence of cervical lymph node metastases, underwent a total thyroidectomy with prophylactic ipsilateral central and level 3 dissection. Level 3 nodes were removed by compartmental dissection or by sampling the sentinel nodes overlying the jugular vein, according to surgeon preference. Data were collected prospectively from January 2011 to August 2014. Statistical analysis was performed by SPSS software.
Results
A total of 137 patients underwent total thyroidectomy with prophylactic ipsilateral central and level 3 dissection for PTC. The incidence of occult level 3 disease was 30 % (41/137 patients). A total of 48 % of patients (66/137) harbored occult central neck disease. A total of 80.5 % of patients with pN1b disease had macrometastases (≥2 mm), and 15 % exhibited skip metastases with central compartment sparing. In patients with pN1b disease, a median of 6 level 3 nodes were retrieved, with an average involved nodal ratio of 0.29. Multivariate regression demonstrated risk factors for occult lateral neck metastasis include tumor size (odds ratio 1.1), upper pole tumors (odds ratio 6.6), and vascular invasion (odds ratio 3.2) (p < 0.05).
Conclusions
PTC is associated with a significant incidence of occult central and lateral nodal metastases. In patients undergoing prophylactic central neck dissection, inclusion of level 3 dissection should be considered in patients with large upper lobe cancers.



Similar content being viewed by others


References
1. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
2. Smith VA, Sessions RB, Lentsch EJ. Cervical lymph node metastasis and papillary thyroid carcinoma: does the compartment involved affect survival? Experience from the SEER database. J Surg Oncol. 2012;106:357–62.
3. Podnos YD, Smith D, Wagman LD, Ellenhorn JD. The implication of lymph node metastasis on survival in patients with well-differentiated thyroid cancer. Am Surg. 2005;71:731–4.
4. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985–1995. Cancer. 1998;83:2638–48.
5. Kouvaraki MA, Shapiro SE, Fornage BD, Edeiken-Monro BS, Sherman SI, Vassilopoulou-Sellin R, et al. Role of preoperative ultrasonography in the surgical management of patients with thyroid cancer. Surgery. 2003;134:946–54.
6. Chan AC, Lang BH, Wong KP. The pros and cons of routine central compartment neck dissection for clinically nodal negative (cN0) papillary thyroid cancer. Gland Surg. 2013;2:186–95.
7. Lee DW, Ji YB, Sung ES, Park JS, Lee YJ, Park DW, et al. Roles of ultrasonography and computed tomography in the surgical management of cervical lymph node metastases in papillary thyroid carcinoma. Eur J Surg Oncol. 2013;39:191–6.
8. Lee SK, Kim SH, Hur SM, Choe JH, Kim JH, Kim JS. The efficacy of lateral neck sentinel lymph node biopsy in papillary thyroid carcinoma. World J Surg. 2011;35:2675–82.
9. Wiseman SM, Hicks WL Jr, Chu QD, Rigual NR. Sentinel lymph node biopsy in staging of differentiated thyroid cancer: a critical review. Surg Oncol. 2002;11:137–42.
10. Ducoudray R, Tresallet C, Godiris-Petit G, Tissier F, Leenhardt L, Menegaux F. Prophylactic lymph node dissection in papillary thyroid carcinoma: is there a place for lateral neck dissection? World J Surg. 2013;37:1584–91.
11. Hartl DM, Al Ghuzlan A, Borget I, Leboulleux S, Mirghani H, Schlumberger M. Prophylactic level II neck dissection guided by frozen section for clinically node-negative papillary thyroid carcinoma: is it useful? World J Surg. 2014;38:667–72.
12. Hartl DM, Leboulleux S, Al Ghuzlan A, Baudin E, Chami L, Schlumberger M, et al. Optimization of staging of the neck with prophylactic central and lateral neck dissection for papillary thyroid carcinoma. Ann Surg. 2012;255:777–83.
13. Park JH, Lee YS, Kim BW, Chang HS, Park CS. Skip lateral neck node metastases in papillary thyroid carcinoma. World J Surg. 2012;36:743–7.
14. Lee YS, Shin SC, Lim YS, Lee JC, Wang SG, Son SM, et al. Tumor location-dependent skip lateral cervical lymph node metastasis in papillary thyroid cancer. Head Neck. 2014;36:887–91.
15. Grodski S, Cornford L, Sywak M, Sidhu S, Delbridge L. Routine level VI lymph node dissection for papillary thyroid cancer: surgical technique. ANZ J Surg. 2007;77:203–8.
16. Randolph GW, Duh QY, Heller KS, LiVolsi VA, Mandel SJ, Steward DL, et al. The prognostic significance of nodal metastases from papillary thyroid carcinoma can be stratified based on the size and number of metastatic lymph nodes, as well as the presence of extranodal extension. Thyroid. 2012;22:1144–52.
17. Zetoune T, Keutgen X, Buitrago D, Aldailami H, Shao H, Mazumdar M, et al. Prophylactic central neck dissection and local recurrence in papillary thyroid cancer: a meta-analysis. Ann Surg Oncol. 2010;17:3287–93.
18. Wang TS, Cheung K, Farrokhyar F, Roman SA, Sosa JA. A meta-analysis of the effect of prophylactic central compartment neck dissection on locoregional recurrence rates in patients with papillary thyroid cancer. Ann Surg Oncol. 2013;20:3477–83.
19. Barczynski M, Konturek A, Stopa M, Nowak W. Prophylactic central neck dissection for papillary thyroid cancer. Br J Surg. 2013;100:410–8.
20. Popadich A, Levin O, Lee JC, Smooke-Praw S, Ro K, Fazel M, et al. A multicenter cohort study of total thyroidectomy and routine central lymph node dissection for cN0 papillary thyroid cancer. Surgery. 2011;150:1048–57.
21. Grant CS, Stulak JM, Thompson GB, Richards ML, Reading CC, Hay ID. Risks and adequacy of an optimized surgical approach to the primary surgical management of papillary thyroid carcinoma treated during 1999–2006. World J Surg. 2010;34:1239–46.
22. Ito Y, Tsushima Y, Masuoka H, Yabuta T, Fukushima M, Inoue H, et al. Significance of prophylactic modified radical neck dissection for patients with low-risk papillary thyroid carcinoma measuring 1.1–3.0 cm: first report of a trial at Kuma Hospital. Surg Today. 2011;41:1486–91.
23. Kang BC, Roh JL, Lee JH, Cho KJ, Gong G, Choi SH, et al. Candidates for limited lateral neck dissection among patients with metastatic papillary thyroid carcinoma. World J Surg. 2014;38:863–71.
24. Kliseska E, Makovac I. Skip metastases in papillary thyroid cancer. Coll Antropol. 2012;36(suppl 2):59–62.
25. Balasubramanian SP, Brignall J, Lin HY, Stephenson TJ, Wadsley J, Harrison BJ, et al. Sentinel node biopsy in papillary thyroid cancer—what is the potential? Langenbecks Arch Surg. 2014;399:245–51.
26. Dralle H, Machens A. Surgical management of the lateral neck compartment for metastatic thyroid cancer. Curr Opin Oncol. 2013;25:20–6.
27. Sywak MS, Learoyd D, Gill AJ, Delbridge LW, Sidhu SB, Clifton-Bligh RJ, et al. Patterns of structural recurrence in papillary thyroid cancer. World J Surg. 2014;38:653–9.
Disclosure
The authors declare no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Fraser, S., Zaidi, N., Norlén, O. et al. Incidence and Risk Factors for Occult Level 3 Lymph Node Metastases in Papillary Thyroid Cancer. Ann Surg Oncol 23, 3587–3592 (2016). https://doi.org/10.1245/s10434-016-5254-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5254-8