
Abstract
The wide range of medical disciplines afferent to anesthesiology (anesthesia, perioperative care, intensive care medicine, pain therapy, and emergency medicine), carry a great, cross-specialty opportunity to influence safety and quality of patients’ care. Operating rooms and Intensive Care Units are settings burdened with a high risk of error: surgery is evolving, while the medical staff working in ICU is expected to provide high-quality care in a stressful and complex setting. It is estimated that about 1.5% of surgical interventions are complicated by critical events, but the true incidence is likely underestimated. Across medical specialties, preventable patient harm is more prevalent in the ICU.
Recommendations and good practices for the safe provision of anesthesia and critical care exist and must be known and transferred into daily practice, since one of the main duties of anesthesia and critical care providers is to provide patient safety. Strategies to reduce the occurrence of medication errors, appropriate monitoring practices, equipment care and knowledge, planification and mastery of non-technical skills during emergencies, as well as designing and sustaining a healthy work environment and adopting adequate staffing policies could have an impact on patient safety and positively influence patient outcomes in this setting. The development of simulation training and cognitive aids (e.g., checklists, emergency manuals) is also changing the approach to crises and is expected to encourage a deeper cultural change.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Medication errors
- Crisis checklist
- Cognitive aid
- Cognitive errors
- Simulation training
- Monitoring
- Depth of anesthesia
- Burnout
- Anesthetic equipment
- Safety culture
- Building factor
- Operating room design
- Communication
- Teamwork
-
Most frequent errors and adverse events in anesthesiology and the intensive care unit (ICU).
-
Strategies to reduce the occurrence of medication errors both in the operating room and in the ICU.
-
Basic principles for the provision of safe anesthesia care: monitoring, knowing, and taking care of the equipment, planning, non-technical skills.
-
Application of cognitive aids to improve the safety of surgical patients. Cognitive aids have been developed for intra- and perioperative crises.
-
Proposals of models aimed at implementing safety solutions.
-
Implications of the psychological status of staff for patient safety and possible interventions.
-
Typical building issues when designing ORs and ICUs.
1 Introduction
Given the wide range of medical disciplines afferent to anesthesiology (anesthesia, perioperative care, intensive care medicine, pain therapy, and emergency medicine), anesthesiologists have always had a great, cross-specialty opportunity to influence safety and quality of patients’ care. In recent decades, several efforts have been made to establish a model of safety and different risk-reduction strategies have been engaged: for example, the establishment of the American Society of Anesthesiologists (ASA) Committee on Patient Safety and Risk Management in 1984 and the birth of the Anesthesia Patient Safety Foundation in the subsequent year, which were significant moments for the improvement of patients’ healthcare quality and for the history of anesthesiology at large.
Indeed, quality and safety in this field have improved, thanks to upgrades of the anesthesia delivery equipment, better monitoring, improved airway management and emergency devices, availability of recovery rooms, and better training; pharmacological advances have led to the development of new receptor antagonists of opioids and hypnotics, and new anesthetic drugs, characterized by shorter and more predictable onset and offset times and fewer side effects. The development of simulation training has changed the approach to crises and contributes to the development of a safety culture beginning in the residency period.
Nevertheless, operating rooms (ORs) and intensive care units (ICUs) remain settings burdened by an extremely high risk of error. Surgery increasingly involves older and sicker patients undergoing more complex interventions; in the meantime, anesthesiologists have been requested to become rapidly competent at using new drugs, devices, and monitoring systems. The situation is not different in the ICUs, where physicians and nurses are expected to provide high-quality care to critically ill patients, often making life-threatening decisions very quickly in a stressful environment while managing high-tech equipment and applying complex procedures.
2 Epidemiology of Adverse Events
A study of reported adverse events under anesthesia [1] estimated that about 1.5% of surgical interventions are complicated by critical events, but the true incidence is likely underestimated; moreover, a systematic review [2] found that surgical and anesthetic adverse events, many of them deemed preventable, contribute to 12.8–52.2% of unplanned ICU admissions. In industrialized countries, major complications are reported [3] to occur in 3–16% of impatient surgical procedures, with permanent disability or death rates of approximately 0.4–0.8%; the anesthesia-specific mortality is estimated [4] to be about 1/100,000 cases. Hence, even if the overall anesthetic risk is estimated to be a small proportion of the total risk of the surgical procedures, with an estimated [5] 312.9 million operations in 2012, anesthesia-related perioperative mortality represents a small but relevant proportion of cases and, given the ubiquity of surgery, the implementation of strategies aimed at improving safety of surgical care has significant implications for public health [3].
Across medical specialties, preventable patient harm is more prevalent in the ICU [6]. ICUs are complex environments where the severity of illnesses, the high levels of stress, the variety of therapies and routes of administration make medical errors and deaths due to preventable harm more common [7]. In the Critical Care Safety Study [8], Rothschild et al. found a daily rate of 0.8 adverse events and 1.5 serious errors for 10 ICU beds, with a rate for serious errors of 149.7 per 1000 patient-days. Notably, 45% of all adverse events were judged preventable.
3 Most Frequent Errors
A recent review [9] suggests that cognitive errors (Table 13.1) are the most important contributors to patient harm in anesthesiology: growing evidence shows that mere technical errors or errors caused by a lack of knowledge account for only a small part of incorrect diagnosis and treatment in this setting. The role of non-technical skills for patient safety has progressively become more evident through the years and, on this topic, one of the most striking moments of reflection for the healthcare community was Martin Bromiley’s report [10] on the death of his wife in 2005. Fixation errors, absence of planification, teamwork breakdown, poor communication, unclear leadership, lack of situational awareness, and other non-technical aspects of performance in anesthesiology and critical care medicine can negatively impact patient outcome. This could be even more relevant during intraoperative crises and emergencies, where failure of adherence to best practices can be common [11].
Another important source of patient harm is represented by medication errors, which can occur at four steps of the drug treatment process: prescription, transcription, dispensation, and administration. As reported by the Anesthesia Quality Institute [12], 44% of medication error claims involve incorrect dosing, 30% substitution of an unintended drug for the correct one, 10% administration of a contraindicated drug, and 8% timing errors. Factors most frequently leading to medication errors or near-misses [13] are distraction (16.7%), haste, stress, or pressure to proceed (production pressure, 12.5%), and the misreading of labels on medication vials or ampoules (12.5%).
Poor design and lack of familiarity with equipment and monitoring devices are likely sources of error and have been identified as major determinants in many adverse events; in this context, the anesthetic delivery equipment is the most common source of problems. Remarkably, equipment misuse is far more common than pure equipment failure, highlighting the fact that human error is responsible for equipment-related mishaps in as high as 90% of cases [14].
Physician burnout and the psychological status of staff are significant concerns for both quality of care and patient safety in critical care. Burnout syndrome has been identified in all categories of healthcare professionals and several studies have shown a high prevalence in ICU staff [15], up to 40%. Risk factors include [16] continuous or long shifts, night shifts, work overload, and poor workplace organization. Healthcare staff who are burned out, depressed, or anxious are unable to fully engage in patient care and are more likely to make errors, increasing the risk to the safety of patients; moreover, burnout personnel may be more reluctant to report medical errors [17]. Depression symptoms were shown to be an independent risk factor for medical error in a prospective observational study [15] involving 31 ICUs.
4 Safety Practices and Implementation Strategies
4.1 Medication Errors
Errors in medication are defined [18] as the mistakes that occur in the drug treatment process and that lead to, or have the potential to lead to, harm to the patient; such errors typically occur when a drug is prescribed, dispensed, prepared, or administered. In a review of more than 10,000 case forms, Cooper et al. [13] reported an incidence of one in 113–450 patients; in ICU, they are reported in a large proportion of incidents, accounting for up to 78% of serious errors [8].
The high-stress, time-sensitive nature of work in the operating room may explain the high risk of medication errors in this setting; consistently, it has been demonstrated [19] that their rate of occurrence for ICU patients is greater than that for patients admitted to general medical wards. In both environments, the high number of drugs and the IV route of administration, which often requires multiple infusion pump setups or calculations of infusion rate, create more opportunities for error. Moreover, the potency of many drugs utilized in these settings (vasopressors and inotropes, strong opioids, general anesthetics) even at small doses increases the risk of harm to critical patients, which typically have little physiological reserve.
Being a substantial, potentially lethal, source of patient harm, several institutions have hence targeted this issue. For example, recently, the European Board of Anaesthesiology has produced recommendations for safe medication practice [20] (Table 13.2).
Chartaceous prescriptions have a high risk of errors due to misinterpretation of handwriting; the use of informatized prescription can surely bring down the number of medication errors due to failure in interpretation. Also, electronic medical records can alert physicians and nurses to potential mistakes (e.g., contraindications, double prescriptions, drug interactions, dilution incompatibilities) and allow a timely documentation of drug administration, granting trackability of every phase of the pharmacological treatment process.
Errors which involve administration of the wrong medication or giving medication to the wrong patient can be reduced by 40% with the implementation of bar-code medication administration technology [21] which matches each and every patient’s electronic order with patient identifiers (wristbands), thus enhancing the adherence to the “five rights of medication administration” (right patient, medication, time, dose, and route).
A critical point in the process is the admission of a patient from the emergency department or the OR to the ICU, and from the ICU to the OR: clinicians should investigate the types of drugs and the lines to which they are infusing. Before the discharge, extreme attention must be paid to vasoactive medications, ensuring that they do not run out during transport. Drug concentrations must be clearly reported and known both precisely and accurately to the ICU personnel, that often has its own dilution protocols, so that pumps can be programmed correctly; in this phase, communication is crucial: a proper sign-out should occur directly between the OR anesthetist and nurses and the ICU physicians and nurses. In the ICU, the adoption of shared dilution protocols could be of help, creating a standard for clinical practice.
4.2 Monitoring
Monitoring is the cornerstone for the provision of a safe anesthesia and a fundamental prerequisite for the effective care of critical patients. In a scientometric analysis, Vlassakov et al. [22] found that the rapid development of anesthesia monitoring may be one possible explanation for the increased safety of anesthesia over the past 40 years.
Standards for basic monitoring during anesthesia have been well established and several guidelines exist. Firstly, ASA [23] highlights that qualified anesthesia personnel shall be present in the room throughout the conduct of all general or regional anesthetics and monitored anesthesia care, mainly because of the rapid changes that may occur in patient status during anesthesia. In the case of a known hazard (e.g., radiation), remote observation is allowed, under the condition that some provision for monitoring the patient is made. Remote observation is also fundamental during radiologic investigations for critical patients.
Basic anesthesia monitoring implies the continuous evaluation of the patient’s oxygenation, ventilation (including capnography), circulation, and temperature during all anesthetics [23]. Nevertheless, technological advancements over the past few years have provided advanced monitoring systems that should be adapted to the different settings and levels of care, mainly depending on a patient’s history and the procedure planned (Fig. 13.1).

In the image to the left an example of monitoring for the operating room; to the right monitoring of the depth of sedation in ICU
Hemodynamic monitoring has evolved considerably, shifting from invasive techniques to less invasive hemodynamic monitoring for the estimation of cardiac output and other measures of circulatory function, both in anesthesia and in the ICU. For example, the use of pulse contour analysis avoids the complications related to a pulmonary artery catheter, while still providing valuable information for effective therapeutic changes.
Noticeably, a useful and quite recent tool that helps anesthesiologists optimize anesthetic administration, both in the OR and in the ICU, is the processed EEG of the frontal lobes (i.e., BIS™—Medtronic, Boulder, CO, USA; Entropy®—GE Healthcare, Helsinki, Finland; SedLine™—SEDline, Masimo Corp., Irvine, CA, USA). Tracking the depth of sedation was highly effective in reducing the risk of intraoperative awareness in 7,761 high-risk patients when compared with guiding the dose based on clinical signs [24]; at the same time, it improves anesthetic delivery, preventing the risk for oversedation and reducing recovery times [25]. This could also be of utmost importance to the ICU, where oversedation is associated with higher rates of ventilator-associated pneumonia and longer ICU stays [26]. In the recent ENGAGES study [27], EEG-guided anesthesia using BIS in elderly patients undergoing major surgery was associated with a significantly lower 30-day mortality and lower intraoperative use of phenylephrine, even though these were investigated as secondary endpoints.
Whenever muscle relaxants are given during anesthesia, the use of a peripheral, neuromuscular transmission monitor (nerve stimulator) is recommended [28] to allow for a rational administration of neuromuscular blocking and reversal agents, and to reduce the risk of residual curarization and its associated complications, as clinical tests alone cannot reliably exclude the presence of residual curarization [29].
Transesophageal echocardiography is mainly a diagnostic tool, but it can provide important information about a patient’s hemodynamic status (preload, cardiac contractility, calculation of cardiac output) and it is estimated [30] that its use in critical patients, together with transthoracic echocardiography, can lead to relevant therapeutic changes in about 25% of cases.
Finally, the efficacy of monitoring for safety may be impaired by poor design and inactivated or inappropriate alarms. Default settings for ventilators, monitors, and alarms should always be checked to determine if they are appropriate [31]. Monitors should clearly display readings and ASA states [23] that alarms should be audible to the anesthesiologist and the anesthesia care personnel. Nevertheless, alarm fatigue is a well-known problem, especially in the critical care setting: excessive false alarms occur frequently and can interfere with clinical activity, contribute to work stress, and desensitize the personnel, leading to a delayed or inadequate response [32]. Several solutions have been proposed (smart alarms taking into account multiple parameters, adaptive time delays, noise reduction strategies, setting of sensible and targeted thresholds) but need to be further investigated.
4.3 Equipment
The care of critically ill patients and patients under general anesthesia is dependent on the use of complex medical equipment; monitoring devices, ventilators, renal replacement therapy machines, extracorporeal circulation technologies, infusion pumps, point-of-care diagnostic tools, each with different designs and characteristics, are increasingly populating the market, adding complexity to the intra- and perioperative settings. Unfortunately, this equipment has the potential to develop faults, to be used incorrectly, or to fail: in the ICU, it is estimated that context equipment and supply issues account for 15.8% of total adverse events [33]; similarly, equipment is involved in approximately 14–30% of all intraoperative problems and the anesthetic delivery equipment is the most common source of problems [14].
Besides the wide range of products available in the market, each anesthesia and critical care provider must be familiar with the products available in the provider’s own setting, including not only their correct use, but also their indications and limits. Anesthesia providers should be aware of the common causes of equipment malfunction and should be trained in the recognition and management of these events. Study and training sessions and on-site training can be useful for this purpose; simulation programs can further reinforce practitioner competency in the use of new equipment and provide experience in the management of common equipment failure in both straightforward and crisis situations, anticipating its occurrence in the real clinical setting [14].
In 2008, ASA updated pre-anesthesia checkout guidelines (PAC) and provided general principles for all anesthesia delivery systems, summarizing checkout tasks to be completed daily and prior to each procedure. Any anesthesia or ICU department should adapt them to their own anesthesia machine design and practice setting [31]. When correctly implemented, PAC can prevent equipment failure and subsequent patient injury; furthermore, it ensures that backup equipment is ready to use in case of intraoperative failures. For example, it is fundamental that a backup machine, an alternative oxygen supply, and manual ventilation devices (Ambu Bag) are always ready to use. In order to meet these requirements and as the responsible party for the proper functioning of all the equipment used to provide anesthesia care [31], anesthesiologists should be competent in performing all the tasks of the PAC.
4.4 Cognitive Aids
It has been demonstrated that cognitive function is compromised as stress and fatigue levels increase, as often happens in the operating room and in intensive care settings, during intraoperative crises and emergencies for example. Here, the complexity of medical conditions and therapies available, the multiple layers of professional roles involved, and the high workload can easily lead to increased errors, decreased compliance with recommended practices, and decreased proficiency in the delivery of care. In this setting, the development of checklists and other cognitive aids has recently risen to prominence and certain procedures or critical events that have been targeted with the use of checklists have shown significant improvements in outcome [34].
Apart from the famous study [35] conducted by Pronovost and collaborators (see the “Building a safety culture” paragraph), another successful application of checklists for the improvement of patient outcomes has been the Surgical Safety Checklist, presented by the WHO in 2008 within the Safe Surgery Saves Lives initiative and developed after a comprehensive consultation with experts in surgery, anesthesia, and other related specialties from across all WHO regions. This checklist was developed with the aim of reducing the occurrence of patient harm [3] in the form of errors and adverse events, and increasing teamwork and communication among surgical team members; it targets a routine sequence of events at three cardinal points of the surgical process: preoperative patient evaluation, surgical intervention, and preparation for postoperative care [3]. The use of surgical safety checklists during routine operative care has been associated with significant reductions in both complications and mortality and has rapidly become a standard of care in the vast majority of countries [36].
The experience of their use in ordinary care has triggered investigations of the potential benefits deriving from cognitive aids in emergency situations; here, time and cognitive resources are limited and it has been demonstrated that the ability to rapidly put in place the right therapeutic interventions is crucial, as outcomes are often time dependent. Moreover, evidence suggests that, during emergencies, failure to adhere to best practices and to recall previously learned protocol is common [11]; in Advanced Cardiac Life Support (ACLS) scenarios, for example, it is known [37] that there is a significant decay in clinicians’ knowledge retention over time after the completion of certification and it has been demonstrated [38] that errors and omissions of indicated steps are associated with decreased survival odds. These premises formed the basis for the development of crisis checklists for the operating room (Fig. 13.2), a type of cognitive aid designed to help the surgical team remember critical steps during intraoperative crises [11]. Some examples are the Anaesthetic Crisis Manual, the Operating Room Crisis Checklists developed at Brigham and Women’s Hospital of Boston, the Stanford Emergency Manual, and the Crisis Management Handbook from the Australian Patient Safety Foundation. Arriaga et al. [36] found that the use of surgical crisis checklists was associated with a nearly 75% reduction in failure to adhere to critical steps in management during operating-room crises in a high-fidelity simulated operating room [11]; these data are consistent with that of Ziewacz et al. [39].

A checklist from the Emergency Stanford Manual
There are also numerous other cognitive aids that have been developed for the perioperative and critical care settings, including ACLS algorithms and anesthesia adaptations for the perioperative setting, Malignant Hyperthermia Association of the United States protocols, a checklist for the treatment of local anesthetic systemic toxicity (LAST) from the American Society of Regional Anesthesia and Pain Medicine, pediatric critical events checklists from the Society for Pediatric Anesthesia, Emergency Neurological Life Support checklists by the Neurocritical Care Society, checklists for the preparation of the operating room, for anesthesia in traumatic patients, and for general emergency protocols, as well as other resources [11].
Globally, many major anesthesia societies support and have adopted cognitive aids [11]: among them the Anesthesia Patient Safety Foundation, the American Society of Anesthesiologists, and the European Society of Anesthesiology. Interestingly, the American Society of Regional Anesthesia and Pain Medicine published in 2010 a practice advisory on local anesthetic systemic toxicity, which included a checklist on the treatment of LAST, and recommended keeping the LAST checklist available in any area where high doses of local anesthetics are used. In 2014, the Society for Obstetric Anesthesia and Perinatology developed a consensus statement on the management of cardiac arrest in pregnancy, recommending that a checklist emphasizing key tasks be immediately available; the American Heart Association encourages institutions to create point-of-care checklists to be used during obstetric crises including maternal cardiac arrest.
4.5 Communication and Teamwork
The connection between safety and communication has been known for a long time. Given the complexity of ICUs and the multiple team handovers required during patient care, critical care units are areas where patients are more vulnerable to communication breakdowns.
The quality of the relationships between nurses, doctors, and other staff working in perioperative settings affects patient outcomes: good teamwork, when team members communicate efficiently and respect each other while working toward a common goal, allows the team to reduce complications and mortality [7]. Conversely, communication failures and bad relationships can lead to increased risk of error, length of stay, resource use, caregiver dissatisfaction, and turnover. In the ICU, the implementation of a daily-goals form can help to set and share tasks and care plans and to improve communication among caregivers [40].
Insight can also be gained from Crisis Resource Management, a well-known approach that refers to all the non-technical skills that have been demonstrated to optimize teamwork and make the teamwork more effective during an emergency. It holds effective communication as one of its key principles [41], underlining the importance of a climate of open information exchange among all personnel.
Simulation training could be a good way to improve relationships and trust within teams and is rapidly becoming part of resident education, even if the relationship between simulation training in anesthesiology and improved outcomes still needs to be clearly defined. In fact, besides helping with technical skills training, simulation can reinforce the non-technical skills needed to work as a team, such as communication behaviors, leadership skills, collaboration, task management, situation awareness, and decision-making [42].
4.6 Building a Safety Culture
The success of many interventions that aim to improve patient safety depends not only on the application of evidence-based practices, but also on changes in workplace culture and on group implemented strategies. Many efforts have been made toward the development of a culture of safety in this discipline, in order to improve patient safety and care quality. Safety culture is the collection of beliefs, values, and norms relating to patient safety and shared among the members of an organization, unit, or team [43]. It influences behavior, attitude, cognition, and one’s perception of one’s own work, promoting safe practices and the prioritization of patient safety over other goals (e.g., efficiency).
The implementation of a safety culture requires sustained involvement across multiple levels of an organization, through a series of steps including the engagement of frontline providers, the selection and creation of team-based projects, the development of safety education programs (including communication and teamwork skills), and the implementation and evaluation of strategies [7]. Despite the fact that its implementation may be a difficult and challenging process (Table 13.3), current evidence [7] supports the efficacy of a strong safety culture in the reduction of adverse events and lower mortality.
One of the clearest examples of successful implementation of safety culture in critical care was the milestone study conducted by Pronovost et al. [35], which reported a large and sustained reduction in rates of catheter-related bloodstream infection in 103 ICUs across Michigan through a quality improvement framework that included:
-
a daily-goals sheet to improve clinician-to-clinician communication
-
training of team leaders across medical and nursing staff
-
a checklist to ensure adherence to evidence-based infection-control practices for central line insertion (Fig 13.3)
Fig. 13.3 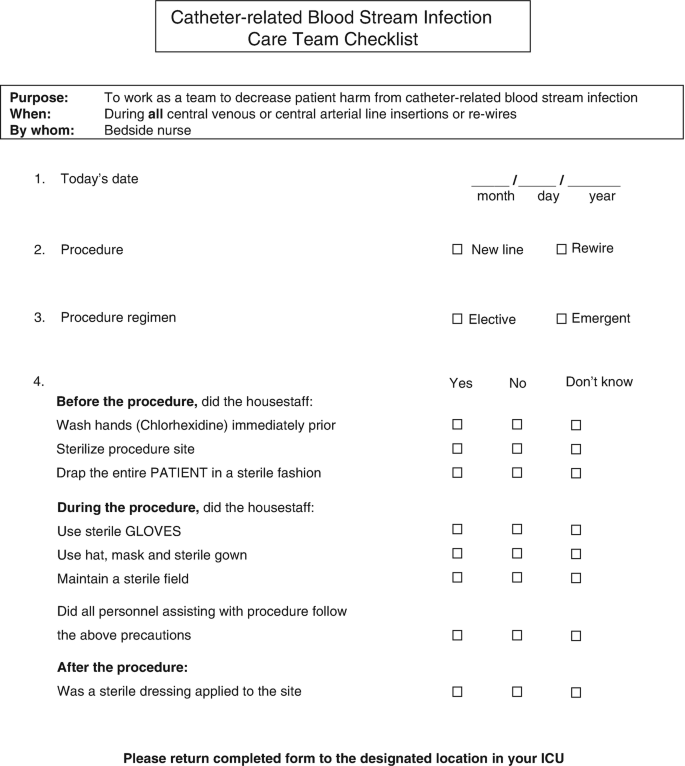
Example of central line insertion checklist
-
empowerment of all ICU staff to intervene in case of non-adherence to any of the aforementioned practices
-
periodic feedback reports
-
tracking and sharing of collected data

Other means of implementation could be interdisciplinary rounding, encouragement of error reporting, and team training; importantly, this includes simulation training. Engaging patients and families in safety culture is deemed important too, since patients can be a relevant source of information in the reporting of adverse events [7].
It should be further considered that financial pressures may lead administrators to limit investments in patient safety improvements, with the additional risk of spreading safety culture problems among the staff. Many aspects of the financial performance of a hospital may lead to hazardous changes in staffing, quality control, physician education, investment in up-to-date equipment, monitoring of adverse events, and may cause other safety issues which eventually may affect patient outcomes. Several pieces of evidence [44, 45] show that there can be a trade-off between financial objectives and patient safety, and that this should be taken into account by a hospital’s administration.
4.7 Psychological Status of Staff and Staffing Policies
Human factors and well-being at work are relevant issues when discussing patient safety. Regarding this topic, burnout syndrome has recently gained popularity: it is a complex, work-related, psychological status, resulting from chronic workplace stress that has not been successfully managed. It is defined in ICD-11 as the combination of:
-
high exhaustion
-
increased mental distance from one’s job or feelings of negativism or cynicism related to one’s job
-
reduced professional efficacy
A variety of interventions have been proposed to address the psychological status of staff and can be divided into two categories [47]: (1) interventions focused on improving the ICU environment; (2) interventions focused on the individual’s ability to cope with the working environment. Multidimensional interventions are more likely than single interventions to succeed in preventing and treating psychological disorders among the staff.
Since 2005, the American Association of Critical Care Nurses has defined [46] six standards to establish and sustain a healthy work environment: (1) skilled communication; (2) true collaboration; (3) effective decision-making; (4) appropriate staffing; (5) meaningful recognition; (6) authentic leadership. Other levels of intervention that have been proposed [47] for a healthy ICU environment are the improvement of end-of-life care and of ethical team deliberations, the utilization of team debriefing, structured communication, the employment of time and stress management skills, interdisciplinary discussions, and the sharing of critical decisions with team members. Family conferencing to discuss prognosis and treatment goals could mitigate moral distress in ICU clinicians.
Intensivist- and nurse-to-patient ratios can also impact patient care and staff well-being, and are associated with improved safety and better outcomes for patients [16]. In 2013, the Society of Critical Care Medicine addressed this issue and published a statement [16] to aid hospitals in determining their intensivist staffing, recognizing that proper ICU staffing impacts patient safety and staff well-being. Assessments of staff satisfaction, burnout, and stress should be part of institution policies. Moreover, staffing policies should factor in surge capacity and non-direct patient care duties (family meetings, consultations, teaching).
Finally, the presence of acute or chronic psychological disorders among healthcare providers, due to private or work-related stress, as well as addiction or substance abuse, sleep disorders, mood disturbance, and overall well-being should be investigated in the context of occupational medicine examinations and should never be underestimated. Critical care providers should be taught how to recognize the risk factors and symptoms for burnout and should be encouraged to seek assistance when needed [47].
4.8 The Building Factor
The environment of operating rooms and ICUs is perceived as static by architects and engineers. Consequently, workplaces are often designed smaller than they actually need to be. For instance, the aisles of the operating rooms should be at least 2 m large to allow the easy and safe transfer of stretchers, but this space is often narrowed by drug carts, echo machines, and other empty stretchers. Similarly, it should be taken into account that the new technologies and devices continuously introduced in clinical practice are usually cumbersome, running the risk of making poorly designed workplaces very uncomfortable [48]. Small ICU rooms may slow down the process of care and hamper the management of critical situations, especially when more clinicians are required.
Relaxation areas or other environments in which the staff may take a break should be considered when planning operating rooms and ICUs, and natural lighting should be guaranteed when feasible [49]. Indeed, breaks should be regularly planned in order to reduce the risk of fatigue and consequently improve the well-being of workers and patient safety. Shifts longer than 8 h should be avoided, and, when this is not possible, adequate recovery time between the shifts should be ensured [50, 51]. For instance, in Italy the employment contract of NHS hospitals includes rules on shift and work breaks, but they are often disregarded in practice.
The regular use of assessment tools [52], such as the Health and Safety Executive’s Fatigue and Risk Index Tool, is paramount to identify workers that are at risk of injury.
5 Recommendations
One of the main duties of anesthesia and critical care providers is to provide patient safety.
Medication error is a substantial source of patient harm in anesthesiology. Recommendations for safe medication practices exist and must be respected. The use of electronic medical records should be favored over chartaceous prescriptions, eventually coupling with bar-code medication administration technology.
A proper sign-out that also addresses medication infusions should occur during the admission to or the discharge from the ICU.
Standards for monitoring have been well established by ASA and are fundamental requisites for the provision of safe anesthesia care since they can detect physiologic perturbations and acute events allowing for intervention before the patient suffers harm. Nevertheless, anesthetist and perioperative physicians should be familiar with advanced monitoring techniques, such as pulse contour analysis, depth of general anesthesia monitoring, neuromuscular monitoring, and transesophageal echocardiography; their use could have important implications for a clinical practice, for example, allowing the rational administration of anesthetic drugs and fluids. As highlighted by ASA, qualified anesthesia personnel shall be present in the room throughout the conduct of all general or regional anesthetics and monitored anesthesia care.
Anesthesia providers must be familiar with the equipment available in their own settings, including not only the equipment’s correct use, but also its indications and limits. Every anesthesia provider should know and be competent in the performance of all the items of the ASA pre-anesthesia machine checklist. Competency in early recognition and management of common equipment failure is a requisite for patient safety.
The WHO surgical safety checklist improves compliance with safety practices and has been demonstrated to have an impact on surgical patient outcome; it is able to prevent patient harm and perioperative complications. The use of cognitive aids during intraoperative crises and emergencies should be encouraged; their use may contribute to better patient outcomes, reducing failure of adherence to the best evidence-based practices and mitigating the effect of stress and ineffective teamwork on performance. Checklists should be integrated into clinical practice through effective training and implementation strategies. Institutions should encourage the creation of adapted point-of-care checklists at critical points of a patient’s treatment in the hospital (e.g., operating room, ICU, obstetrics).
Simulation training of critical events need to be incorporated into the education of all clinicians who work in the operating room and in the ICU. Anesthetists should receive this type of formation since residency. Simulation training should include the use of crisis checklists and emergency manuals, and the simulation of equipment failure.
Efforts should be made to establish a culture of safety in critical care, as safety culture could promote effective improvements in patient safety and sustain them over time. Efforts should be conducted at a multidisciplinary level including administrations, while engaging patients and families in this process is also deemed important. Reporting of errors and adverse events should be encouraged and collected data should be tracked and shared among the personnel. Hospitals’ financial plans should include investments in patient safety since overlooking this aspect may increase the probability of adverse patient safety events.
Institutions should regularly assess the appropriateness of their ICU staffing models via objective data. Critical care providers should be taught how to recognize the risk factors and symptoms for burnout and should be encouraged to seek assistance when needed. Policies of routine screening of ICU staff members for symptoms of depression, burnout, and anxiety should be implemented.
The size, layout, and organization of the workplace impacts staff well-being and patient safety. It is crucial that administrators, architects, and engineers involve lead clinicians and focus on input from clinical staff when designing operating rooms and ICUs.
References
Charuluxananan S, Punjasawadwong Y, Suraseranivongse S, et al. The Thai anesthesia incidents study of anesthetic outcomes II. Anesthetic profiles and adverse events. J Med Assoc Thail. 2005;88:S14–29.
Vlayen A, Verelst S, Bekkering GE, et al. Incidence and preventability of adverse events requiring intensive care admission: a systematic review. J Eval Clin Pract. 2012;18(2):485–97.
World Health Organization. World alliance for patient safety—safe surgery saves lives. Geneva: WHO; 2008. https://www.who.int/patientsafety/safesurgery/knowledge_base/SSSL_Brochure_finalJun08.pdf.
Staender SE, Mahajan RP. Anesthesia and patient safety: have we reached our limits? Curr Opin Anaesthesiol. 2011;24(3):349–53.
Weiser TC, Haynes AB, Molina G, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015;385:S11.
Panagioti M, Khan K, Keers RN, et al. Prevalence, severity, and nature of preventable patient harm across medical care settings: systematic review and meta-analysis. BMJ. 2019;366:I4185.
Thornton KC, Schwarz JJ, Gross AK, et al. Preventing harm in the ICU—building a culture of safety and engaging patients and families. Crit Care Med. 2017;45(9):1531–7.
Rothschild JM, Landrigan CP, Cronin JW, et al. The critical care safety study: the incidence and nature of adverse events and serious medical errors in intensive care. Crit Care Med. 2005;33(8):1694–700.
Stiegler MP, Neelankavil JP, Canales C, et al. Cognitive errors detected in anaesthesiology: a literature review and pilot study. Br J Anaesth. 2012;108(2):229–35.
Bromiley M. The case of Elaine Bromiley: Clinical Human Factors Group; 2005. p. 1–18.
Hepner DL, Arriaga AF, Cooper JB, et al. Operating room crisis checklists and emergency manuals. Anesthesiology. 2017;127(2):384–92.
Sandnes DL, Stephens LS, Posner KL, et al. Liability associated with medication errors in anesthesia: closed claims analysis. Anesthesiology. 2008;109:A770.
Cooper L, DiGiovanni N, Schultz L, et al. Influences observed on incidence and reporting of medication errors in anesthesia. Can J Anaesth. 2012;59(6):562–70.
Dalley P, Robinson B, Weller J, et al. The use of high-fidelity human patient simulation and the introduction of new anesthesia delivery systems. Anesth Analg. 2004;99(6):1737–41.
Garrouste-Orgeas M, Perrin M, Soufir L. The Iatroref study: medical errors are associated with symptoms of depression in ICU staff, but not burnout or safety culture. Intensive Care Med. 2015;41(2):273–84.
Ward NS, Afessa B, Kleinpell R, et al. Intensivist/patient ratios in closed ICUs: a statement from the Society of Critical Care Medicine Taskforce on ICU staffing. Crit Care Med. 2013;41(2):638–45.
Halbesleben JR, Rathert C. Linking physician burnout and patient outcomes: exploring the dyadic relationship between physicians and patients. Health Care Manag Rev. 2008;33(1):29–39.
Pharmacovigilance Risk Assessment Committee. Good practice guide on recording, coding, reporting and assessment of medication errors (EMA/762563/2014). European Medicines Agency. 2015.
Wilmer A, Louie K, Dodek P, et al. Incidence of medication errors and adverse drug events in the ICU: a systematic review. Qual Saf Health Care. 2010;19(5):e7.
Whitaker D, Brattebø G, Trenkler S, et al. The European Board of Anaesthesiology recommendations for safe medication practice. Eur J Anaesthesiol. 2017;34(1):4–7.
Thompson KM, Swanson KM, Cox DL, et al. Implementation of bar-code medication administration to reduce patient harm. Mayo Clin Proc Innov Qual Outcomes. 2018;2(4):342–51.
Vlassakov KV, Kissin I. A quest to increase safety of anesthetics by advancements in anesthesia monitoring: scientometric analysis. Drug Des Devel Ther. 2015;9:2599–608.
American Society of Anesthesiologists. Standards and Practice Parameters Committee. Standards for basic anesthetic monitoring. 2011. https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring.
Punjasawadwong Y, Phongchiewboon A, Bunchungmongkol N. Bispectral index for improving anaesthetic delivery and postoperative recovery. Cochrane Database Syst Rev. 2014;6:CD003843.
Chhabra A, Subramaniam R, Srivastava A, et al. Spectral entropy monitoring for adults and children undergoing general anaesthesia. Cochrane Database Syst Rev. 2016;3:CD010135.
Hajat Z, Ahmad N, Andrzejowski J. The role and limitations of EEG-based depth of anaesthesia monitoring in theatres and intensive care. Anaesthesia. 2017;72:38–47.
Wildes TS, Mickle AM, Abdallah AB, et al. Effect of electroencephalography-guided anesthetic administration on postoperative delirium among older adults undergoing major surgery: the ENGAGES randomized clinical trial. JAMA. 2019;321(5):473–83.
Gelb AW, Morriss WW, Johnson W, et al. World Health Organization-World Federation of Societies of Anaesthesiologists (WHO-WFSA) international standards for a safe practice of anesthesia. Can J Anaesth. 2018;65(6):698–708.
Lien CA, Kopman AF. Current recommendations for monitoring depth of neuromuscular blockade. Curr Opin Anaesthesiol. 2014;27(6):616–22.
Vignon P, Mentec H, Terre S, et al. Diagnostic accuracy and therapeutic impact of transthoracic and transesophageal echocardiography in mechanically ventilated patients in the ICU. Chest. 1994;106(6):1829–34.
Sub-Committee of ASA Committee on Equipment and Facilities. Recommendations for pre-anesthesia checkout procedures. 2008. http://asahq.org/standards-and-guidelines/2008-asa-recommendations-for-pre-anesthesia-checkout.
Ruskin KJ, Hueske-Kraus D. Alarm fatigue: impacts on patient safety. Curr Opin Anaesthesiol. 2015;28(6):685–90.
Corwin GS, Mills PD, Shanawani H, et al. Root cause analysis of ICU adverse events in the veterans health administration. Jt Comm J Qual Patient Saf. 2017;43(11):580–90.
Hales BM, Pronovost PJ. The checklist—a tool for error management and performance improvement. J Crit Care. 2006;21(3):231–5.
Pronovost P, Needham D, Bernholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006;355(26):2725–32.
Arriaga AF, Bader AM, Wong JM, et al. Simulation-based trial of surgical-crisis checklists. N Engl J Med. 2013;368(3):246–53.
Semeraro F, Signore L, Cerchiari EL. Retention of CPR performance in anaesthetists. Resuscitation. 2006;68(1):101–8.
McEvoy MD, Field LC, Moore HE, et al. The effect of adherence to ACLS protocols on survival of event in the setting of in-hospital cardiac arrest. Resuscitation. 2014;85(1):82–7.
Ziewacz JE, Arriaga AF, Bader AM, et al. Crisis checklists for the operating room: development and pilot testing. J Am Coll Surg. 2011;213(2):212–7.
Pronovost P, Berenholtz S, Dorman T, et al. Improving communication in the ICU using daily goals. J Crit Care. 2003;18(2):71–5.
Goldhaber-Fiebert SN, Howard SK. Implementing emergency manuals: can cognitive aids help translate best practices for patient care during acute events? Anesth Analg. 2013;117(5):1149–61.
Green M, Tariq R, Green P. Improving patient safety through simulation training in anesthesiology: where are we? Anesthesiol Res Pract. 2016;2016:1.
Weaver SJ, Lubomsky LH, Wilson RF, et al. Promoting a culture of safety as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 Pt 2):369–74.
Encinosa WE, Bae J. Health information technology and its effects on hospital costs, outcomes, and patient safety. Inquiry. 2011;48(4):288–303.
Bazzoli GJ, Chen HF, Zhao M, et al. Hospital financial condition and the quality of patient care. Health Econ. 2008;17(8):977–95.
American Association of Critical-Care Nurses. AACN standards for establishing and sustaining healthy work environments: a journey to excellence. Am J Crit Care. 2005;14(3):187–97.
Moss M, Good WS, Gozal D, et al. A critical care societies collaborative statement: burnout syndrome in critical care health-care professionals. A call for action. Am J Respir Crit Care Med. 2016;194(1):106–13.
Ibrahim AM, Dimick JB, Joseph A. Building a better operating room: views from surgery and architecture. Ann Surg. 2017;265(1):34–6.
Berry K. Operating room architecture and design and the effects on staff morale. ACORN J. 2008;21(2):6–16.
Banakar M. The impact of 12-hour shifts on nurses’ health, wellbeing, and job satisfaction: a systematic review. J Nurs Educ Pract. 2017;7(11):69–83.
Ferri P, Guadi M, Marcheselli L, et al. The impact of shift work on the psychological and physical health of nurses in a general hospital: a comparison between rotating night shifts and day shifts. Risk Manag Healthc Policy. 2016;9:203.
Noone P, Waclawski E. Fatigue risk management systems needed in healthcare. Occup Med. 2018;68(8):496–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2021 The Author(s)
About this chapter

Cite this chapter
Damiani, S., Bendinelli, M., Romagnoli, S. (2021). Intensive Care and Anesthesiology. In: Donaldson, L., Ricciardi, W., Sheridan, S., Tartaglia, R. (eds) Textbook of Patient Safety and Clinical Risk Management . Springer, Cham. https://doi.org/10.1007/978-3-030-59403-9_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-59403-9_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-59402-2
Online ISBN: 978-3-030-59403-9
eBook Packages: MedicineMedicine (R0)