
Abstract
This case describes the application of quality improvement to improve services provided at the community level to the most vulnerable children (MVC) in the community, those orphaned or affected by HIV. The case describes the experience of supporting local communities in Tanzania to implement the QI approach outlined in Tanzania’s National Most Vulnerable Children QI Guidelines. In particular, the case focuses on start-up activities needed to get the initiative up and running, including gaining buy-in from community leaders, determining baseline performance, mobilizing MVC committees to serve as QI teams to test changes to care processes, and supporting shared learning across teams. The case also speaks to the particular challenges as well as benefits of implementing QI at the community level.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
- Collaborative Improvement
- Community Health Workers
- Community-Based Organizations
- Most Vulnerable Children
- Orphans and Vulnerable Children
- Shared Learning
- Tanzania
Background and Setting
In Tanzania, the Department of Social Welfare (DSW) of the Ministry of Health and Social Welfare is responsible for guiding and coordinating interventions to ensure the care, support and protection of most vulnerable children (MVC). MVC are defined as children who are 18 years old or younger, who live in high-risk circumstances, and whose prospects for continued growth and development are seriously impaired. MVC, including those who are affected by and living with HIV, are vulnerable to chronic diseases, developmental delays, and reduced educational opportunities, as well as potential abuse, stigma, and discrimination from their family members, caregivers, and communities.
The 2012, the Republic of Tanzania Population and Housing Census (PHC) estimated the number of MVC in the country at 3,000,000. However, the 2012 National Indicator Survey revealed that 1.3% of children below 19 years old are HIV positive and that 9.4% had had their first sexual encounter before the age of 15. Around 37% of children in this age group reported at least one episode of sexual violence, while 23% reported an episode of physical violence. Like all vulnerable population groups, MVC struggle to access basic services, such as education, adequate food, shelter, and social and psychosocial support. To bridge the access gap, the DSW developed the National Costed Plan of Action (NCPA) for Most Vulnerable Children I (2007–2010). The Plan sought to establish a community-driven response to strengthen households’ and communities’ capacity to care for, protect, and support MVC who are HIV-positive or affected by HIV.
Developing and Communicating Standards for MVC Care and Support
In 2009, the DSW led development of the National Quality Improvement Guidelines for Most Vulnerable Children (National MVC QI Guidelines) to standardize and improve the quality of services provided by various stakeholders. The guidelines covered eight service areas:
-
Food and nutrition
-
Shelter
-
Family-based care and support
-
Social protection and security
-
Primary health care
-
Psychosocial care and support
-
Education and vocational training
-
Household economic strengthening
The National MVC QI Guidelines shifted MVC program priorities from distribution of commodities to ensuring an improved quality of life. Guidelines defined stakeholders’ roles and responsibilities and specific standards for quality improvement (QI) of each of the eight service areas, including desired outcomes, essential actions, illustrative activities, best practice notes, and quality indicators.
The DSW sought to disseminate the National MVC QI Guidelines in a way that would ensure that stakeholders would understand and implement its principles. The department called upon a donor-funded project to develop a training package to facilitate communication of the guidelines to service providers throughout the country’s health-care system, from the village to the national level.
In 2010, the DSW published the Training Package for Improving Quality of Care, Support, and Protection for MVC in Tanzania, which standardized training procedures to guide implementation of the national guidelines. The DSW and project staff trained 39 national facilitators, who in turn trained government representatives and implementing partners involved in care, support, and protection of MVC at regional and district councils in 19 regions.
Following the training, the DSW set up a demonstration site by focusing on intensive implementation of the guidelines in one of the districts.
Organizing the Improvement Effort
Actors at the Village Level
In Tanzania, the government administrative system is comprised of national, regional, district (council), ward, and village or hamlet levels. The village or hamlet, the closest point to the household level, is where MVC beneficiaries interact with entities and groups which provide care, support, and protection services, including community-based organizations, government social and health services, and local nongovernmental organizations (NGOs). These organizations and groups include district- and village-level MVC committees, village authorities, community health workers, support groups, and households.
MVC committees play a critical coordination role in providing services to MVC. The DSW provides guidance and criteria for the formation of MVC committees and selection of members. The community, during an open public meeting, uses a participatory approach to nominate and select MVC committee members. To support this selection process, the community development officer (CDO) or any designated government official from the ward level provides guidance on qualifications. The MVC committee’s main role is to coordinate all interventions related to care, support, and protection of MVC in that community.
While the MVC committee plays a leading role in service coordination, other players at the village level also are critical to the provision of services. The village authority, a government entity, oversees all village activities, including resource mobilization for MVC to access services. Community health workers—village residents who have undergone basic health training—play key roles by monitoring the growth and general health of under-five children, including MVC. Volunteer groups, such as savings and internal lending groups, women’s groups, and faith-based organizations, sometimes play a role in resource mobilization and in supporting MVC to access various services.
District Selection
The DSW was aware, as a result of observations gained from their own supervisory visits and feedback received from partners, that MVC committees had been largely ineffective in organizing and supporting MVC to access quality services. MVC committees had inadequate understanding of their role and were not effectively utilizing available local resources. The DSW requested that a United States Agency for International Development (USAID)-funded QI project provide technical support to effectively train providers at the primary service level to understand and implement the National MVC QI Guidelines.
Since improving care for MVC was a new activity, the DSW and the USAID-funded QI project decided to start by supporting improvement activities on a small scale, in three wards of one demonstration district. The main objective of the demonstration was to engage those involved in caring for MVC to understand and apply standards stipulated in the National MVC QI Guidelines.
The DSW and project staff reviewed a range of options to select the location best suited to serve as the demonstration site. Not all districts in the country had active MVC programs, so the DSW opted to choose a district where services were already being provided. Bagamoyo District, where UNICEF had already started initiatives to support MVC activities, emerged as a top choice. In addition, it was a rural district which was relatively close to Dar es Salaam, where the project office was located making it easier to monitor. Bagamoyo District was eager to expand on its current MVC activities and had a social welfare officer (SWO) committed to the effort, so it was decided to move forward with this district. At the time, there were a total of 169 districts in Tanzania; Bagamoyo was one of the six districts in the Pwani Region.
Collaborative Improvement
The project and DSW staff agreed that a collaborative improvement approach would be the most appropriate and effective way to organize teams and improvement activities for this initiative. Collaborative improvement brings together multiple teams working on the same improvement aims in order to share experiences, foster peer-to-peer learning, and spread successful changes rapidly across all participating teams.
Collaborative improvement serves as a way to organize and leverage the efforts of multiple teams. Teams use plan-do-study-act cycles to test the effectiveness of changes implemented at their sites. On a regular basis, usually every 3–5 months, all teams in a ward or district are brought together in a learning session to share the changes they have tested and their results. They compare and learn from each other’s efforts, both successful and unsuccessful. Following the learning session, team members take successful ideas back to their own improvement efforts and adapt and test changes using additional plan-do-study-act cycles. Throughout this process, the community’s quality improvement teams are supported by coaches who provide feedback, guide data collection and analysis, and help teams carry out the steps in the plan-do-study-act cycle.
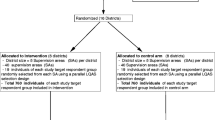
The demonstration involved all key stakeholders working in Bagamoyo on MVC services, including representatives from the DSW, the regional health management team, council staff, nongovernmental organizations, community-based organizations, ward and village authorities, and MVC committees. Start-up and implementation involved a series of steps and activities, which are summarized in Fig. 10.1 above. This case study describes each of these steps in detail.

Timeline of activities
Initial Introductory Visits
In October 2010, staff from the DSW, the USAID-funded QI project, the Regional Health Management Team in Pwani, and the implementing partner conducted an initial site visit to Bagamoyo District to hold discussions with district authorities to gain their support and to create a working relationship with key stakeholders in the district. This visit, the first of a series arranged by the DSW, provided an opportunity to learn and understand how the district’s MVC program worked.
The planning group was comprised of five people, each with a specific role: two project staff provided technical assistance on how to put QI into action, the DSW gave technical guidance on policy and national guidelines, the implementing partner’s representative described MVC activities, and the Regional SWO provided guidance on how to translate policy into implementation at the council level. Government standards encouraged projects and implementing partners to involve Ministry level staff in first visits.
The visit involved a series of meetings with a few representatives from targeted departments and organizations within Bagamoyo District, such as a visit to a local NGO that provided MVC services. The planning group held discussions with the district’s SWO to explore the district’s engagement and identify gaps in community structures and services.
Planning group members conducted an introductory visit with district authorities, including the council health management team, which plays a primary role in the coordination and supervision of all health-related activities, and the district executive director. The meeting was intended to help officials recognize where their missions and goals overlapped and to identify areas in which they were able to collaborate. The district executive director reported that the meeting shed light on how improvement activities fit within their mandate to ensure that all vulnerable groups have access to various services. This initial visit enabled them to draw up a plan and begin key activities to launch the improvement collaborative.
In addition, the planning group conducted interviews with children and guardians to informally collect qualitative information. This data collection was continued during the baseline assessment. The group interviewed not only six informants from council departments, giving priority consideration to social welfare, but also the education and community development departments. They met with two local service providers and nine ward officers, three from the Ward Executive Officers, three from community development, and three from education.
When group members compared notes, they found that concerns focused on several key areas: MVC committee functionality, MVC data quality, the role of the SWO, and budget support for MVC. At the end of visit, the planning group analyzed and employed the information and began to plan implementation of MVC improvement activities.
The planning group noted performance gaps with respect to DSW guidance, particularly pertaining to communications and relationship dynamics between the village authorities and the MVC committees. They found that the MVC committees were inadequate reporting to the village authorities, and the village authorities, in turn, were inadequate providing guidance and support. In addition, the interests of the MVC committees and village authorities appeared to conflict. The MVC committees lacked updated and consistent data and information; for example, their data registrars were incomplete and out-of-date. Further, the MVC committees did not have plans in place to provide support services to MVC and were not linking them to services. The planning group conducted a feedback meeting for the head of the Community Development Department and the district-level SWO. The information was also presented at the first district-level learning session.
Ward Selection
The planning group worked with council staff from the social welfare and community development departments to identify and select wards to participate in pilot improvement activities. In searching for pilot sites, the group took into consideration a range of criteria in order to achieve a well-rounded sample. They searched for sites that would provide a balance of rural and urban areas and that had a high concentration of MVC. They also focused on sites that had current MVC data as well as those where volunteers were actively working. They gave primary consideration to sites that had existing community structures which were supported by other implementing partners.
The SWO provided basic information about the wards, including the number of MVC and the number of MVC committees, and records of previous trainings and interventions. The planning group and council staff chose three out of the 22 wards in Bagamoyo District for the pilot improvement activities. The three wards included the Dunda Ward, with its 22 hamlets; Fukayosi Ward, located in a rural setting, with four villages; and the rural Kiwangwa Ward, with five villages. The three wards had a total of 463 MVC (Kiwangwa, 154; Fukayosi, 98; and Dunda, 211). At the time of the intervention, Bagamoyo District had 5504 MVC, of which 2904 were males and 2600 were females. The district’s SWO held discussions with the ward authorities from each location, including the executive, community development, and ward education officers, all of whom agreed to participate in improvement activities.
District and Ward Start-Up
In March 2011, the DSW and project staff conducted advocacy meetings at the district and ward levels. Specifically, the DSW and project staff held a 1-day meeting in each ward to explain the project’s objectives and approach to authorities. The objectives were to explain the roll-out of activities and to determine appropriate coaches at the district and ward levels.
The DSW and project staff provided district and ward leaders with guidance and made recommendations regarding selection of coaches. Coaches would support the improvement teams by providing a variety of services:
-
Acting as mentors to team participants on all aspects of the improvement process (team formation, problem analysis, and conducting plan-do-study-act cycles), as well as data collection and analysis
-
Providing training on MVC guidelines
-
Serving as advocates and intermediaries with higher levels of government on how to address larger systemic problems
The district-level SWO and community development officer (CDO) were largely responsible for selecting district coaches. They chose representatives from the Social Welfare, Community Development, Education, Health, and Planning departments, as well from nongovernmental and faith-based organizations. In total, about 10–12 representatives served as district coaches over the course of the project. The district coaches’ primary responsibilities were to coordinate and coach ward and village teams and to ensure allocation and mobilization of resources at the district level across all sectors.
In addition, the district SWO, in collaboration with the ward executive officer, selected ward-level coaches. They chose individuals from departments that had an oversight role for MVC or MVC services, such as the education or community development department. Ward-level coaches were community development officers, education coordinators, executive officers, and agriculture extension officers. These coaches were responsible for guiding MVC committees at the village level, overseeing all activities within the villages, and serving as a key link between the village and district levels. All information moving between the district and villages passed through the ward coaches.
Two of the coaches, one from an NGO and one from a faith-based organization, received funding from an implementing partner to provide MVC services. Based in the wards, the two coaches were able to work with the teams on a day-to-day basis to help them identify gaps and find ways to address them. The two coaches stayed with the project for a few years until funding for their organizations ran out.
Baseline Assessment
In January 2011, the first major activity was to conduct a baseline assessment in the three wards and associated villages and hamlets. The project staff, with input from the DSW, designed a simple questionnaire with key questions targeting services areas and indicators stipulated in the national guidelines. Baseline survey respondents included MVC parents or guardians and the children themselves. Project staff, together with Bagamoyo’s Department of Social Welfare and social welfare officer, conducted a one-day orientation meeting for 13 volunteers who were identified by local implementing partners and paid to participate in the data collection. At the end of the session, each data collector was allotted, based on the number of MVC they oversee within their residential areas, a number of respondents to interview. Two project staff, the SWO, and a Ministry of Health and Social Welfare representative served as supervisors.
Questionnaires were administered to MVC beneficiaries and to parent or guardian caregivers to elicit information on the MVC and their perspectives on the quality of services provided. Project staff received information on 367 respondents (85.7% of the 428 MVC registered in the three wards) of whom 180 were female and 187 were male. Data on 340 MVC were used for analysis.
The findings were presented at the first district-level learning session to give teams an understanding of the current level of ward performance and to select improvement priorities. In May 2011, following the first learning session, village-level QI teams collected their own baseline information using a subset of the indicators.
The results of the original and QI team baseline surveys are shown in Table 10.1. The two baseline surveys showed large discrepancies. One explanation for the discrepancies is that volunteer data collectors may have been affected by a desire to portray the results in the best light possible. By the time the teams collected their own baseline numbers, they had updated registries and had perhaps better understood the improvement process and the value of honest reporting. The largest identified gaps appeared in the area of services for vulnerable children under 5 years of age, the result of many service providers focusing primarily on providing education services for older children. As a result, primary school enrollment was at 100%. Going forward, the project used the team baseline as the more reliable source of information.
Team Formation
The project staff, working together with the DSW, determined that since the MVC committees existed for coordinating MVC activities at the district, ward, and village levels; no parallel or new system should be created. Instead, project staff worked with the SWO and executive officers from each ward and village to assess how well their MVC committees were functioning. When necessary, an MVC committee added members that would bring useful skills, functions, experience, and perspective to the committee. For example, an MVC committee added as a member a home-based care provider who was able to link children to MVC services and caregivers to treatment adherence support. Also invited to join the committee was a village extension officer who oversaw agricultural development to help with issues of household economic strengthening. The criteria for adding new members included selection and acceptance by a village assembly (which occurred at open community meetings), a clean criminal record, and residence within that village or hamlet. By adding additional members and responsibilities, the MVC committee went from an entity that coordinated activities to a QI team responsible for improving the quality of care of MVC support and protection services.
Initially, the council MVC committee planned to conduct improvement activities at their own level. The council MVC committee was trained in quality improvement, but only some four or five members remained on the committee. Members served as coaches, but no district-level improvement activities took place.
A total of 25 MVC committees were strengthened to implement QI in nine villages and 16 hamletsFootnote 1 in three wards. Each village or hamlet had one MVC committee consisting of 10–12 members, including community health workers and a community justice facilitator. Members also included influential community members, such as, representatives from religious organizations (primarily Muslim and Christian), caregivers, vulnerable children aged 12 years or older (one boy and one girl), and teachers.
In villages where there was MVC committee turnover due to relocation, dropouts, or deaths, the village authority replaced them by following the selection procedures and guidance laid out by the DSW.
Capacity Building
The first learning session, held in April 2011 and organized by project, DSW, and Regional Health Management Team staff, introduced district, ward, and community MVC committees to key policy issues, offered guidance on MVC programs, and provided QI training. In addition, the session was intended to help participants reach mutual agreement on how improvement activities would be carried out. During learning sessions, MVCC reviewed topics, such as planning actions, setting aims and goals, identifying initial changes for improvement, and selecting indicators. Four learning sessions were held: one for the district level and one for each of the three wards.
First Learning Session at District Level
Facilitators from the project and implementing partners, the DSW, and the regional SWO conducted the first 3-day learning session for 30 members of the district-level MVC committee in Bagamoyo township. The participants were from council departments and representatives from local non-governmental organizations who were involved in supporting the district’s MVC services. The session, held at participants’ work stations, was cost-effective as transportation and accommodation costs were not incurred. The location also conveyed a sense of ownership among participants. The main aim was to train participants on the detailed content of the National MVC QI Guidelines and their application to planning and budgeting processes. The objectives of the learning session were to:
-
Orient district staff on the national guidelines for MVC programs
-
Introduce the concept of QI in MVC service delivery
-
Explain the collaborative improvement approach at the community level
-
Create a common understanding of roles and responsibilities in the implementation of QI activities
The facilitators trained participants on the model for improvement and plan–do–study–act cycles. Participants learned how to guide ward coaches and village MVC committees on how to identify existing quality gaps, develop and test changes, and measure for improvement. Some of the key training topics included the following:
-
Identifying the factors that make services effective
-
Recognizing how stakeholders can implement QI in MVC services
-
Understanding QI guidelines and approaches
-
Organizing QI activities
-
Measuring changes in MVC wellbeing
The facilitators emphasized the use and strengthening of existing structures and systems at the community level for implementing the National QI Guidelines in MVC service delivery.
District participants were expected to provide supportive supervision to ward and village teams, as well as to develop improvements (changes to test) in their own work. For example, they chose to improve coordination between the social welfare and education departments in the use of MVC data for service support.
First Learning Session for Community Level
To build QI capacity, the DSW officer, project staff, and ward authorities, with support from the national and regional levels, organized a 3-day learning session for the MVC committees from each ward. Five members of each team participated in the learning sessions, including the chairperson, secretary, community health worker, community justice facilitator, and village executive officer. The learning session was held within the participants’ ward on community premises, such as a school or ward hall.
The trainings have been very helpful because we were just doing things in our way, we had no knowledge to identify MVC needs and address them on the set standards because we didn’t recognize that there were certain standards to be followed. But now we know what we are supposed to do, we can plan and also act accordingly. QI team member, Bagamoyo District
The DSW and project staff trained the MVC committees on the National MVC QI Guidelines by using the training package designed for this purpose. Facilitators focused on building participants’ understanding of the MVC service standards in each of six core service areas: food and nutrition, shelter and care, education, health, protection, and household economic strengthening. In addition, they were also oriented on key national plans and existing MVC policies, such as the National Costed Plan of Action (NCPA) II, 2010–2013.
Facilitators then taught the participants how to improve their performance in achieving those standards by analyzing their own systems and processes for MVC service delivery, identifying and testing changes in the organization of care that could result in improved quality and efficiency, and using data to document and understand the effect of changes.
At the end of the learning session, each MVC committee came up with a plan to address initial issues based on their own performance gaps or problems identified through the training exercises. The plans included the key challenge/problem, activities to address the problem, responsibilities of different actors, and a timeline. Following the learning session, each team collected their own baseline for the key indicators.
Carrying Out the Improvement Work
Following the learning session, the MVC committees took the first step by updating their own community data. Most vulnerable children (MVC) data consists a range of variables: the number of MVC in a village; demographic data, such as age, sex, and location of residence; data on the needs of each child; and the caregiver’s information. The MVC committees carried out visits to all MVC homes to collect this information and update their records to serve as a baseline.
Each MVC committee reviewed data for the eight improvement areas and determined which one or two areas they would start with. During the meetings, teams discussed the service areas and related key essential actions from the guidelines to determine which needed improvement. The teams compared the needs of the registered children with the essential actions to identify the biggest gaps. They used this information to develop their improvement aims. The teams then discussed the key issues and gaps and those which most significantly affected their local services. They developed several possible goals and then narrowed the list down to a few with which to begin. Each team agreed on their own aim based on the vulnerable children’s priority needs. The village executive officer and ward coaches provided guidance to their teams on how to set goals based on ideas received from team members. They discussed which steps were needed to implement, essential actions, and who or which group should be involved. They then tested their plan for changes using plan-do-study-act cycles.
…As I am speaking we have mobilized TSH 335,000 to support children with various services … such as paying school fees for two secondary children, and we have other four children who are doing exams this year and they have special session at their school so they don’t break for lunch hours to go home rather all parents have contributed for food to be prepared at school, so we have paid that contribution for lunch for these four children … we want them to concentrate so they can perform well and their health not to deteriorate. Reported by QI team member, Bagamoyo
The team agreed to monitor their changes using indicators selected from the National MVC QI Guidelines. After indicators were selected, they tasked each team member with visiting children and providing feedback both during regular meetings and with QI team members who lived nearby. In some cases, teams created their own indicators to track and test specific changes, for example, the number of MVC visited by MVC committee members each month.
Organization of MVC Committee Meetings
MVC committees conducted regular meetings to discuss progress and goals. While most MVC committees conducted monthly meetings, some teams conducted them every 2 months or even twice per month, depending on priorities and tested changes. Each MVC committee met in a variety of venues within their village: at village authority offices, in schools, or in any available community building. Sometimes they chose informal areas to meet, such as under a tree in the village authority office area. In some cases, meetings were held at the houses of team members, depending on agreement of members, convenience, and availability of space. The MVC committee chairperson convened the meetings, and either the team secretary or village executive officer facilitated discussions. The chair was responsible for ensuring that all agenda items were discussed and that consensus was reached on next actions.
Examples of changes implemented in three service areas and their results are shown in Table 10.2.
Documentation
MVC committee secretaries kept records of all meetings, including notes on all key issues. To ensure that team members were in consensus and because not all members were literate, the secretary read the minutes aloud. The records included notes covering the committee’s planned actions, as well as their accomplishments and challenges encountered. Meeting records were used to discuss plans, goals, and challenges with coaches. Teams kept their own records in notebooks and/or put information into a documentation tool provided by the project.
After we came from the training/learning session we agreed with teams to go and update MVC data, we were sure most of the data were not updated so even the number of MVC were not realistic hence it will be difficult to implement improvement plans without knowing how many MVC are existing and what are their specific needs. So the first aim was to support teams to review their MVC data.
Ward education coordinator, Bagamoyo
To facilitate the recording of information, the documentation tool covered key topic areas and provided as an annex, a summary of the National MVC QI Guidelines’ eight core service areas for easy reference:
-
MVC services
-
Names of team members attending meeting
-
Performance self-ranking on MVC service provision (poor, average, good, and best)
-
Challenges
-
Planning matrix to address challenges/gaps in QI, objectives, key changes or activities, indicators, and baseline data
-
Successes to be shared
We are now speaking the same language and using same data source. For example, if we want to support MVC through our budget line, we don’t follow our own way to get names of MVC as before, but we communicate together with the SWO to ensure consistency and get names of MVC to support through MVC registers and MVC committee but not any other source.
District staff, Bagamoyo
As copies of the documentation tool were not alwayas readily available, many teams also kept counter books (notebooks) to record meeting notes. Most of the records were kept at village authority offices or by the secretary or chairperson to be easily accessed when village offices were closed. Some teams kept records of communications with village authorities.
Data Collection
Data recorded in the MVC registers were updated by following DSW procedures. The existing reporting framework required information to travel from the village (MVC committee) level through wards to the districts. However, information was not always disseminated as the reporting framework required. The project facilitated data collection while on site visits and passed on the reports.
The DSW had provided MVC registers to keep all data updated for a particular village. Prior to initiation of the QI effort, these registers had been updated only every 6 months following a process of initial identification of new MVC and updating information for existing children. The data in a register was open for official use to any service provider who was planning to conduct an intervention in that village. The MVC committee frequently used the data to plan support, such as determining which children were eligible to have school fees paid. The teams used the register to complete their indicator matrix at the end of each month to document accomplishments and actions taken. The matrix was used by all levels to review and analyze performance in a given service area.
Since we have done thorough updating of data, we now know our MVC and we have the plan to support them such as starting with providing birth certificates to all 13 children … according to previous data we had 20 MVC, but it took us long and we did not take it serious, from that we discovered some children have moved out from our village.
– Village executive officer, Bagamoyo
The introduction of QI facilitated the collection and reporting of information at the village, ward, and district levels. Team members began recording services provided to children as they took place rather than waiting for the biannual report. These records were then compiled into monthly and quarterly reports. Government reports are routinely done on quarterly basis to be sent to the ward level and then to the district. However, MVC committees updated data in the indicator matrix each month to ensure that services were accurately documented.
At the meetings at the end of each month, the teams also filled out the indicator matrix as shown in Table 10.3.
Teams also made a second copy of data records which included items, such as, the number of MVC and their names, ages, gender, school status, services received, and which organization delivered them. They kept these duplicate records as a backup and to be able to get quick access to basic information without having to go to the village office.
Teachers or village executive officers would often help other team members, whose educational levels varied, to understand the data.
Support for Improvement Teams
Coaching visits were scheduled to allow teams time, between visits, to implement planned activities and document key successes, accomplishments, and challenges. The initial coaching visit was held 4–5 weeks after the first learning session and aimed at reminding teams of what they learned at the first learning session. The visit was also intended to support teams to revise their initial implementation in coordination with a wider group of stakeholders from the village.
The main objective of ongoing coaching was to strengthen the capacity of MVC committees to implement their planned priority actions. National and regional coaches provided policy guidance and updated district coaches and teams on national issues related to MVC programming. They also provided guidance and feedback on implementation of teams’ plans and analysis of data. District coaches provided immediate, ongoing technical support and guidance through visits and calls. They linked QI team members with stakeholders, when appropriate.
It has been more than six months since we submitted requests for birth certificates for our children at the district office, we are following up and we are not sure what is happening, if you can find out for us since you are also coming from the district that will be great. A QI team member, giving a message to the district coach
District coaches got ready for visits by preparing a letter, accompanied by any relevant documents, to inform ward authorities of the planned visit, including its objectives, expected attendees, date, and place. Due to time and resources, two or three QI teams met jointly and shared with coaches the challenges in implementing changes and QI action plans, as well as their achievements. Coaching sessions lasted between 2 and 3 hours. During these visits, a representative of each QI team, often the chairman or secretary, would present on which of the planned actions had been accomplished. They also presented on how challenges were addressed and their upcoming plans and strategies. Members of other teams were given an opportunity to comment and ask questions.
Coaches supported teams in the following ways:
-
Reviewed accuracy of data and provided guidance on filling out data collection forms. For example, teams were initially unclear about how to read numerators and denominators so the coaches helped team members understand them.
-
Explained each component of the documentation tool and reviewed how to fill it out.
-
Reviewed guidelines and key actions with team members.
-
Shared experiences and best practices from other Tanzanian programs to provide teams with ideas for plans and activities.
-
Explained team roles and fostered teamwork.
-
In order to maximize community resources, encouraged team members to create a network of providers and use it to make referrals.
-
Encouraged team members to support each other.
-
Suggested that teams create saving and loan groups that caregivers could also join.
One area that coaches focused on was helping team members to distinguish between which improvement work fell under the control of the MVC committee and which should be referred to other services and organizations. They reviewed, with committee members, existing support and service networks and emphasized the importance of providing referrals since MVC committees did not provide direct services. They reviewed how to link and refer children and caregivers to various services, especially those that required skilled providers, such as HIV testing and counseling and/or legal assistance. Coaches kept notes on teams’ progress in order to follow up on achievements and challenges. Challenges which fell outside the team’s purview sometimes needed to be brought to the attention of district-level authorities. For example, the committees would refer wide-ranging issues, such as MVC not accessing free government-provided medical services despite having community health fund cards which proved eligibility.
The coaching process empowered MVC committee members, extension workers, and district staff to improve processes by providing guidance on use of the plan-do-study-act cycle and application of National QI Guidelines. The approach of bringing two or three teams together for joint coaching allowed teams to share experiences and solutions and learn from one another. It also created a healthy competition between teams. One team member from a village in Kiwangwa Ward acknowledged that their performance was low compared to the ward’s other five teams, saying: “We can’t allow other villages to be on top of us, because we can also do that and make things better. Next time you visit us you will see changes in our team”.
The first coaching visits were held in June 2011, with visits conducted each month until July 2012. Visits were then conducted only for poorly performing teams as needed through June 2015.
One example of a successful knowledge exchange occurred when the Mkenge village team presented during the second coaching visit on how they were able to obtain birth certificates for all 13 MVC in the village. The birth certificate, a document critical to MVC, is used to access and enroll in educational and other services. The Fukayosi team learned from the presentation that relationships between village authorities and community members had been key to the success of the Mkenge team. By the time the third coaching visit took place in September 2011, about 4 months after starting improvement work, the Fukayosi team reported that, by mobilizing resources together with village authorities, they had obtained birth certificates for all 55 MVC in their village.
Second Learning Sessions for MVC Committees
In November 2011, 6 months after the first learning session was held, a second round of learning sessions gave teams a chance to share their progress and experiences with other communities. National and regional coaches from the DSW, project, implementing partners, and the regional health management team facilitated the district learning session. Coaches from the district staff, with support and backup from national coaches, facilitated community-level learning sessions for the community level.
One of the learning sessions was focused on building the capacity of ward and district coaches to provide regular technical assistance to QI teams. The session offered opportunities to talk about implementation experiences, review teams’ progress, and share strategies.
A 2-day learning session held at each ward for the MVC committees and ward coaches allowed teams to present on goals, actions taken, results, and challenges. The session’s objectives were to engage teams in analyzing and implementing actions for change and to facilitate sharing challenges and successes according to their priority areas. Teams prepared progress reports on achievements, key changes implemented, challenges faced, and ways in which they overcame them. In addition, teams requested guidance from peers and coaches on obstacles which they had not yet surmounted.
Teams learned ways of improving care from listening and talking to each other. The friendly competition between villages (described above under Support for Improvement Teams) resulted in the Fukayosi team producing another improvement. The team became motivated to use the project’s documentation tool after listening to how the Mkenge team was using it to update data and record key priorities. The Fukayosi team began to document all activities, including communication faith-based organizations and village authorities. They also started to use a counter book to record meeting activities in case they were unable to access the documentation tool.
Results
The collective results of the village teams are shown in Fig. 10.2.

Results from five indicators monitored by QI teams
Sustaining Improvements and Spread
Six months after the three initial wards started work in October 2011, MVC committees in six new wards were trained in quality improvement and began implementation. In July 2012, an additional 13 wards were added, leading to full coverage of Bagamoyo District. By the end of 2012, all 22 wards were participating in learning sessions and receiving coaching visits. These newly trained MVC committees were able to quickly adopt and implement the successful change ideas from the initial demonstration sites.
Challenges
Coaches and MVC QI teams faced an ongoing challenge of turnover among team members. Because this work was done on a voluntary, unpaid basis, committees and coaches often found that members’ own activities and work took precedence. Sometimes, team members had relocated. Some teams broke up, and the village authority had to assemble new teams. Ward coaches regularly checked on the teams’ performance as part of their ongoing supervisory duties, even when they were in the village for other reasons. Three teams had to be reorganized with only one or a few of the original members remaining. Coaches and team members then faced the challenges of transferring knowledge to and developing improvement skills in new team members. These changes often happened at the same time as leadership changes at the village level, especially when new leaders were not aware of how to carry the work forward.
Myself I always visit villages for different work related to education, on the cause of that I make time to chat out with some members whom I will meet and checking on the progress. For example, during the visit I was informed one girl was forced to a marriage, left school at standard 6, and she was 15 years. I had two strategies with the QITs, where a visit to family was done, and we had to send the representative of QITs with the police. … All things went well and this child is back to school. And I have assigned one teacher to continue to provide psychosocial support to this girl so that she become normal with school life. Ward Education Coordinator, Bagamoyo
One example shows how a team was able to get back on track after losing all but one of its original members. The MVC committee in one hamlet of Dunda Ward had been rated as the most effective of 16 teams. In December 2014, the team collapsed; at the same time, new leadership took over at the hamlet. These changes led to the formation of a new team with only one of the former members remaining. The team requested support from ward coaches, specifically the Community Development Officer and the Ward Education Coordinator, to orient the new members in QI. Five months later, in June 2015, DSW and project staff, during a coaching visit, found that the team had effectively recovered: keeping data up-to-date and mobilizing 335,000 TZS (roughly 150 USD) for MVC services.
Competing government development priorities also influence sustainability. Infrastructure development, such as, building and rebuilding health facilities, classrooms, and roads and bridges, was given higher priority than providing social services. As one district coach noted: “We really advocate for community members to support MVC, but whenever the priority comes such as building of classroom all the directions change … also our budget is limited compared to priorities”.
Reflection
Reflection from Team Members
Team members reported that working with community leaders and government institutions, such as village authorities and schools, helped teams reach their goals. The village chairperson successfully exercised influence to bring support through advocacy activities. The village executive officers also helped guide teams to plan and implement changes.
If the community is involved to know the problem facing it, it can cooperate to help to overcome that problem. For example, we are now aware of the vulnerable children, they were there before but we didn’t care. But we have been empowered and sensitized. We are confident and ready to continue with what [the project] has facilitated.
QI team member, Bagamoyo
Teams acknowledged that ongoing capacity building provided through learning sessions and coaching led members to reach a consensus and share understanding about the approaches and actions to take to provide quality MVC services. Members reported that capacity building efforts were motivational. When asked for one action they would have done differently, team members shared that they would have, from the project’s beginning, engaged ward councilors in meetings or coaching sessions. Although councilors had not been fully engaged in early activities, they had proven key to the improvement effort. Because they serve as decision makers and approve budgets for the district council, they provided invaluable guidance in how resources could be effectively allocated to MVC and caregivers.
Reflection from the Author
The work of this collaborative demonstrates how an MVC committee, whose members are well trained, can effectively apply service standards to improve the quality of MVC services. The introduction of improvement approaches engaged existing MVC committees to function as improvement teams and motivated and empowered them to address gaps in meeting national standards. QI activities equipped team members with the knowledge and skills needed to provide quality services to vulnerable children. In addition, MVC committees began collaborating with other stakeholders to provide services that would meet priority needs. A critical lesson the MVC committees learned was that involving families and caregivers in providing and coordinating care is critical to effective delivery of MVC services. This concept was spread to other districts beyond Bagamoyo.
Frequent external coaching, especially from district officials, motivated members to continue to be actively engaged in continuing to work to improve MVC services. Teams found that coaching and involving local leaders, teachers, and community development officers were key to supporting teams to translate standards into practice.
As teams collected data and analyzed indicators related to specific service standards, they developed a deeper understanding of the standards. Coaches encouraged MVC committees to reflect on their achievements in order to instill in them the confidence to reevaluate and modify plans when goals were not being reached. In addition, coaches found creative ways to provide guidance, such as comparing indicator performance to routine occurrences, to explain more complex QI areas. For example, they might ask: “If your child received a 0 out of 10 on an exam, would that be good? Likewise, you don’t want a child to receive 0 out of 10 services”. Eventually, MVC committee members were able to use indicators to assess their performance and, in turn, present data to advocate for resources. MVC committees disaggregated data by sex and age, which facilitated provision of improved services that corresponded with the needs of individual children. This approach was started in Bagamoyo and spread to all teams.
Services have very much improved and the QI teams are working hard to provide services to vulnerable children. They follow up vulnerable children to make sure they get all necessary services. The communities didn’t recognize the importance of birth certificates but now they do. The QI teams also know the importance of data for decision making and planning. They know how many MVC they have, how many have been helped to get certain services, and how many still need services. District Officer, Bagamoyo
Results produced by the demonstration sites showed that educating, sensitizing, and raising community awareness is a necessary first step in generating a positive response to improving the quality of programs. MVC committees led efforts to educate and sensitize other community members, including leaders, about the community’s responsibility in supporting vulnerable children. Ward and district coaches needed to regularly follow up and encourage accurate and complete documentation and generate sharing of changes and best practices.
The experience of the MVC collaborative improvement initiative showed the importance of including and engaging community leaders in improvement processes. The Bagamoyo teams were at the forefront of the effort to ensure that the needs of vulnerable children were met and their rights recognized. Village chairpersons, not immediately recognizing their role and potential for contribution, were not initially involved in the effort. MVC committee members agreed that chairpersons should be included in all coaching visits in order to provide guidance on matters, such as community and resource mobilization. Thereafter, community leaders grew more active in participating in MVC committee meetings. The implementation of QI activities has facilitated the social welfare office to coordinate services with other council sectors during the planning process and to mobilize resources across sectors at the council level.
The MVC committees also enhanced public–private partnerships by engaging stakeholders, such as, shop owners, hotel owners, and farmers to support MVC to access various services. MVC committee members live in the communities they are serving, thus ensuring sustainability of improvement. The MVC committees, through learning sessions and coaching, acquired the skills and knowledge to plan and implement changes. Village authorities took active roles in supporting MVC committees, allocating resources, and involving community members in supporting vulnerable children. Coaches at the district and ward levels internalized the QI principles and guidelines which assisted them in planning technical support to MVC committees and ward and village authorities.
Notes
- 1.
The term hamlet, vitongoji in Swahili, is used in small township areas and is equivalent to village.
Acknowledgements
The author expresses gratitude to Eveline Kamote, Principal Social Welfare Officer of the Ministry of Health and Social Welfare of Tanzania, and to Sayuni Hizza, District Social Welfare Officer, Bagamoyo. Jared Mussanga, QI Advisor, and Kim Stover, Senior Improvement Advisor, of University Research Co., LLC both contributed in important ways to improve the quality of services for most vulnerable children in Tanzania and the contents of this case. The activities described to improve the quality of services for most vulnerable children in Tanzania were made possible by the generous support of the American people through USAID and its Applying Science to Strengthen and Improve Systems (ASSIST) Project, managed by University Research Co., LLC under Cooperative Agreement Number AID-OAA-A-12-00101.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2020 University Research Co., LLC
About this chapter

Cite this chapter
Nyagawa, F.P. (2020). Strengthening Services for Most Vulnerable Children Through Quality Improvement Approaches in a Community Setting: The Case of Bagamoyo District, Tanzania. In: Marquez, L. (eds) Improving Health Care in Low- and Middle-Income Countries. Springer, Cham. https://doi.org/10.1007/978-3-030-43112-9_10
Download citation
DOI: https://doi.org/10.1007/978-3-030-43112-9_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-43111-2
Online ISBN: 978-3-030-43112-9
eBook Packages: MedicineMedicine (R0)