
Abstract
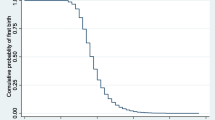
In Indian State of Uttar-Pradesh, there is always pressure among newly-wed to conceive early and have births. Research studies have documented relationship between age at first birth & fertility, besides the socio-demographic factors that influence them. Study aims answering such relationships by the use of frailty models. Indian fertility is characterized as too-early-too-fast. By age-30 majority women would have completed the childbearing. Forty percent of the women had first birth below 18 while 95% experienced before reaching age 26. Births at younger age are reflection on poor enforcement of child-marriage restraint act-18 for girls & 21 for boys. The data is from NFHS-3[3]. The frailty model capturing the unobserved heterogeneity in the event time is preferred over the standard survival models. For the current study, inverse Gaussian with log-logistic baseline-hazard is used, as it fits the data well. Age at marriage and women’s literacy significantly determines the Age at First Birth. The model also predicts significant frailty with variance parameter 0.11
Similar content being viewed by others

Avoid common mistakes on your manuscript.
I. Introduction
The age of women at which they have first child has important consequences on the demographic characteristic of the population [4]. Lower the age at first birth implies higher rate of fertility and population growth because of the shorter length of time between generations [6]. Teenage pregnancies and birth are substantial health risks both for the mother and the child [8]. Adolescent child-bearing restrict growth of mother’s educational attainment resulting in reduced economic opportunity and participation in the labour market for the mother as-well-as the household [2] [5]. There is a strong relationship between age at first birth and children ever born to women. Early childbearing results in large number of children compared to those who start late [1] [5]. Early initiation of childbearing lengthens the reproductive period and subsequently increases fertility. In developed economies, postponement of first births-due to an increase in the age at marriage, has contributed greatly to overall fertility decline. The relationship between age at first birth and fertility is studies extensively and has been well documented. This study aims to answer whether or not the age at first birth is influenced by socio-demographic factors and if yes to know the direction of such influences using frailty models. Scope: In a traditional Indian society and a demographically backward state of Uttar Pradesh with fertility rate still above three plus children there is immense families/societal pressure among newly wed couples to bear children. Not able to produce children immediately after marriage is perceived as women being in-fecund. This negatively impact family’s social standing in the community/society. It is therefore very important to revisit the socio-demographic differentials so as to study the society’s norms on marriage and child bearing. Indian government has legislated legal minimum age at marriage for boy (21 years) and girls (18 years). However, enforcement of this particular law is amongst the worst in the country. Demographically, backward states of Uttar Pradesh, Madhya Pradesh, Rajasthan and Bihar still have large proportions of girls getting married below the legal minimum. This study aims to revisit the strength of association between age at first birth and socio-demographic factors in light of frailty models. Instead of constant baseline hazard the log-logistic distribution is assumed with Inverse-Gaussian frailty.
II. Data and methods
The study utilizes the Date from India’s National Family Health Survey round three conducted by Macro International and International Institute of Population Sciences under the auspices of Ministry of Health and Family Welfare, GOI. The survey covered a wide range of data regarding demography and health of individual women and children besides collecting information on couples as well. Complete reproductive history including fertility of individual women and health status of the individual women aged 10-49 were collected. From the raw data set we have selected a cohort of married women aged 30-34 years for the current analysis as by this age each woman gets married and experiences the event of child bearing. A sample of 1641 women belongs to this cohort. The target fertility variable under study is the age of women at the time giving first birth. A set of socio-demographic variables has been selected for determining influencing factors to the women’s age at first birth. The central focus of the analysis is the frailty models with survival time data i.e., time to event data. A short description of survival analysis with parametric baseline hazard is presented below. Let,
T – Response, time to failure
xt – Row vector of covariates
[T |xtβ] – Some density f (t)
-
Survival analysis is characterized by censoring and truncation
-
It is much more convenient to think in terms of survival function S(t) = P (T > t) and hazard function h(t) = f (t)/S(t), i.e. instantaneous probability of failure given survival up to t.
-
Response is actually the triple (t0, t, d) where subject observed from (t0, t] and either failed (d = 1) or was censored (d = 0). The covariates in the model are assumed constant over (t0, t].
The proportional hazard assumes the form; h(ti) = h0(ti) exp(xi tβ) for some baseline hazard h0(t).
The cox-regression is a proportional hazard model that makes no assumption about the functional form of h0(t). Under the parametric survival model instead we assume some functional form for h0(t). For the current study we assume that the age at first birth episodes follows a log-logistic distribution which takes the form
Here a = exp ( - A ∝ ) and b = exp ( - B ß ) alpha and beta are the model parameters to be estimated. While A & B are the first component of the covariate row vectors and are equal to one.
The parametric specification plus covariates can only go so far in explaining the variability in observed time to failure. The excess unexplained variability is an over-dispersion which is caused either by model misspecification or omitted covariates. This led to the development of frailty models. A frailty model attempts to measure this over -dispersion by modeling it as resulting from a latent multiplicative effect on the hazard function, i.e. the hazard becomes h(t|α) = α h(t). From the proportional hazards perspective, it is easy to see how ‘α’ may correspond to an omitted covariate (or set of covariates).
In this study we assume distribution of alpha as Inverse Gaussian having density and survival function as
The unconditional survival function is given by;
For further details on frailty model one can refer to Wienke, A. [7]. Description on the dependent and selected independent variables used in the analysis is provided below.
Dependent variable: Age at first birth is the dependent variable and it ranges between 12 and 34. Therefore outcome variable under the survival setting is
- Yi :
-
= Age of women at first birth.
Covariates
- X1 ::
-
Age at first marriage of women
- X2 ::
-
Place of residence
- X3 ::
-
Literacy status of women
- X4 ::
-
Religion
- X5 ::
-
Ever use of contraceptives
- X6 ::
-
Caste
- X7 ::
-
Household Wealth Index
The study analyzes the data using frailty models. Before incorporating frailty variables into the survival models, the parametric proportional hazard method of survival analysis is performed using log logistic distribution.
III. Findings and discussion
The characteristics of the sampled women aged 30-34 is presented in the table 1 below. The distribution of age at first birth is slightly skewed as is reflected in the graph below. The majority of women experience birth of first child between ages 15-24. About 72 percent of the sampled women aged 30-34 got married by age 18 the legal minimum for girls. Sampled women are predominantly Hindus (79%) and live in rural areas (58%). More than half of the sampled women (59%) are illiterate. Only about 10 percent of the sampled women had education levels beyond secondary school. Twenty three percent of the sampled women belonged to SC/ST category while 46 percent of the women belonged to other backward caste category. Thirty one percent of the women belonged to general caste category. Twenty four percent of the women never used any method of contraception while about 74 percent of the women did use any method of contraception which includes both modern as well as traditional. Forty one percent of the sampled women belonged to either poorest or poorer categories, while 43 percent were richer or richest. About 16 percent of the women belonged to middle income group (q3 quintile).
Table 2 below shows the mean and median survival duration of the women’s selected characteristics, those literate, marrying at higher ages, belonging to other caste (other than SC/ST & OBC) and are from high socio-economic strata are more likely to give their first birth at higher ages than their respective counterparts. The mean and the median survival duration are computed only for those variables that are used in the Cox Hazard model in table 3.

Table 3 below presents findings from the Cox-survival model with constant baseline hazard function. Prior running Cox model the proportionality assumption for each covariate under study was examined. The place of residence, religion and the ever use of contraception was dropped from the analysis as they do not meet the proportionality criterion. The Log-log plot is presented through graphs at Appendix. In the final run education, age at marriage, caste and the wealth index were used to fit the cox proportional hazards model. Respondents who are literate have 24 percent less likely to have age at first birth at age which illiterate women would like to have, the difference is statistically significant. Similarly, women marrying ages 15-19 are 58 percent less likely to have age at first birth at which women of ages 8-14 years have their first birth. As the age of women increases higher percentages are less likely to have age at first birth at which women of age 8-14 have. The difference is statistically significant. Caste is not statistically significant in explaining the survival difference in age at first birth. No significant difference in age at first birth was found either by wealth quintiles or the socio-economic category to which the respondent belongs.
Table 4 below presents findings from the parametric survival model were-in the baseline hazard function for age at first birth follows the log-logistic distribution. We also try to capture unobserved heterogeneity in survival time by incorporating Inverse-Gaussian frailty. The age of women at their first birth may be affected by the factors those are not considered in the analysis. Some of these factors are unobservable.
For example age at marriage significantly determines age at first birth. However, there are many cultural considerations that determine age at marriage such as dowry, socio-economic status of respondent’s family, individual attributes such as beautifulness etc. cannot be precisely incorporated in the model, it is therefore wise to model individual frailty. As the parametric form is assigned to the baseline hazard function we run the model incorporating full set of covariates. The coefficients are more or less in the same direction as in the case of Cox-Survival model, however a non zero shape parameter (gamma) justifies the use of parametric form for baseline hazard function. Similarly, the hypothesis that the estimate of variance is zero if rejected pointing towards unobserved heterogeneity. It is therefore parsimonious to use the log-logistic parametric form with inverse Gaussian Frailty rather than simple Cox Survival Model.
IV. Conclusion
Age at marriage and women’s literacy is the most significant factor explaining variations in age at first birth. Also The shape parameter value of 0.055 (gamma) under log-logistic baseline hazards reflects better fit than constant baseline hazards. The Inverse-Gaussian frailty with non-zero variance estimate of θ=0.11 reflects significant unobserved heterogeneity in the Age at First Birth.
Acknowledgement
Authors would like to thank MOHFW, GOI New Delhi for supporting the study
References
Bumpass, L.L, Rindfuss, R. and Janosik, R.B. 1978. Age and Marital Status at First Birth and the Pace of Subsequent Fertility. Demography, 15(1): 75–86.
Haque, A.M. and Sayem, A.M. 2009. Socioeconomic Determinants of Age at First Birth in Rural Areas of Bangladesh. Asia Pacific Journal of Public Health, 21(1): 104–111.
IIPS and Macro International. (2007). National Family Health Survey-3: 2005-06 International Institute for Population Sciences, Mumbai, India
Rajaretnam, T. 1990. How Delaying Marriage and Spacing Births Contributes to Population Control: An explanation with Illustrations. Journal of Family Welfare, 36: 3–13.
Rao, K.V. and Balakrishnan, T.R. 1988. Age at First Birth in Canada: A Hazard Model Analysis. GENUS, 44: 53–72.
Teachman, D.J. Heckert, D.A. 1985. The Declining Significance of first birth Timing. Demography, 22: 185–198.
Wienke, A. 2011. Frailty Models in Survival Analysis. Taylor and Francis Group, LLC, London, Newyork.
Zabin, L. and Kiragu, K. 1998. The Health Consequences of adolescent sexual and fertility behavior in Sub-Saharan Africa. Studies of Family Planning, 29: 210–232.
Author information
Authors and Affiliations
Additional information
Authors’ profile
Ajay Pandey is an Assistant Director with Population Research Centre, in the Department of Economics, University of Lucknow, Lucknow, Uttar Pradesh, India.
Dr. Dilip C Nath is a Professor of Statistics at Department of Statistics, University of Gauhati, Assam, India.
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Appendix: Proportionality Check
Appendix: Proportionality Check

a) Education Category (0=Illiterate 1=Literate)

b) Religion Category (1=Hindu 2=Others)

c) Place of Residence

d) Wealth Index

e) Age at First Marriage (AgeM 8/14=1, 15/19=2, 20/24=3, 25/29=4, 30/34=5)

f) Ever Use Contraception ()=Never Used, 1=Traditional Method 2=Modern Method)

g) Caste (1=SC/ST, 2=OBC, 3=Others)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made.
The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
To view a copy of this licence, visit https://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pandey, A., Nath, D. Frailty Approach to Age at First Birth in Uttar Pradesh-India. GSTF J Math Stat Oper Res 3, 4 (2015). https://doi.org/10.7603/s40836-015-0004-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.7603/s40836-015-0004-9