
Abstract
Protein tyrosine phosphatases (PTPs) play an important role in regulating cell signaling events in coordination with tyrosine kinases to control cell proliferation, apoptosis, survival, migration, and invasion. Receptor-type protein tyrosine phosphatases (PTPRs) are a subgroup of PTPs that share a transmembrane domain with resulting similarities in function and target specificity. In this review, we summarize genetic and epigenetic alterations including mutation, deletion, amplification, and promoter methylation of PTPRs in cancer and consider the consequences of PTPR alterations in different types of cancers. We also summarize recent developments using PTPRs as prognostic or predictive biomarkers and/or direct targets. Increased understanding of the role of PTPRs in cancer may provide opportunities to improve therapeutic approaches.
Similar content being viewed by others
Signaling pathways are coordinately controlled by a balance between activators, such as protein tyrosine kinases (TKIs), and inactivators, including protein tyrosine phosphatases (PTPs). To date, cancer biology and drug development has primarily focused on TKIs, with relatively little understanding about the contribution of PTPs to regulate signal transduction in cancer cells[1–3]. In the human genome, the 107 PTPs can be divided into four families according to differences in the amino acid sequence of catalytic domains and in evolutionary development: class I cysteine-based PTPs, class II cysteine-based PTPs, class III cysteine-based PTPs, and Aspbased PTPs. The largest family of the four, the 99-member class I cysteine-based PTPs, can be further grouped into two subfamilies: tyrosine-specific, or classical, PTPs, which include 21 receptor-type PTPs (PTPRs) and 17 non-receptor PTPs (NRPTPs); and VH1-like dual-specificity phosphatases, which are more diverse and contain substrates in addition to pTyr[4].
In this review, we focus on the 21 PTPRs (including PTPRA, PTPRB, PTPRC, PTPRD, PTPRE, PTPRF, PTPRG, PTPRH, PTPRJ, PTPRK, PTPRM, PTPRN, PTPRN1, PTPRO, PTPRQ, PTPRR, PTPRS, PTPRT, PTPRU, PTPRZ, and PTPRZ1), which are largely homologous in structure and function. PTPRs consist of a transmembrane domain, unequal number of extracellular domains, and intracellular catalytic domains. Immunoglobulin-like domains and fibronectin type III-like domains comprise the extracellular domain of many PTPRs. Twelve of the 21 PTPRs have two catalytic domains arranged in tandem. The catalytic activity mainly resides in the membrane-proximal domain (D1) for many PTPRs with the exception of PTPRA, whose membrane-distal domain (D2) also has some activities[5]. For other PTPRs, the D2 domain has been reported to play an important role in maintaining the stability of the whole protein and regulating protein dimerization[6].
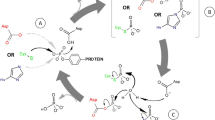
PTPRs are tightly regulated in cell signaling by a variety of mechanisms including post-translational modifications and/or dimerization[7–9]. Reversible oxidation is another important mechanism for regulating PTPR activity. The invariant cysteine residue in the active site of PTPRs has a low pK α , which makes it susceptible to oxidation[10] In PTP1B, the sulfenic acid, which is displayed when the cysteine is oxidized, is converted to a cyclic sulfenamide structure to prevent further irreversible changes of cysteine to sulfinic or sulfonic acid[11]. The inactive sulfenamide structure can be reverted to cysteine with reducing agents, thus providing a reversible mechanism of PTPR activation.
Tyrosine phosphorylation has a crucial role in the regulation of physiological processes such as cell proliferation, differentiation, adhesion, and migration, which are closely relevant to human diseases, especially cancer. Genetic and epigenetic alterations such as copy number changes, mutation, and promoter methylation contribute to the expression level and/or function of PTPR proteins. Numerous PTPRs are reported to be involved in a variety of cancers[12]. Although PTPRs share similar basic structures and the conserved cysteine in active sites, individual PTPRs have specific targets and thereby play different roles in cancer. This review focus on the impact of PTPR alterations across a spectrum of cancers and the clinical implications of targeting PTPRs therein.
Genetic and Epigenetic Alterations of PTPRs
Genetic alterations that are frequently seen in cancers include mutation, copy number loss/deletion, and copy number amplification. Gain-of-function mutations can increase the activity of an oncogene, and loss-of-function mutations may silence a tumor suppressor gene. Of the 21 PTPRs, 20 are mutated in multiple cancers, per The Cancer Genome Atlas (TCGA) data (summarized in Figure 1 ). Mutation appears to be the most common mechanism by which PTPRs are genetically modified when compared with copy number amplification or loss.

Receptor-type protein tyrosine phosphatase (PTPR) genetic alterations In cancer. Three genetic mechanisms were reported in the Cancer Genome Atlas (TCGA): mutation (green), deletion (blue), and amplification (red). Alterations of 20 PTPR family members are summarized across 25 human cancers studied to date (all TCGA, provisional), including skin cutaneous melanoma, lung adenocarcinoma, gastric adenocarcinoma, bladder urothelial carcinoma, lung squamous cell carcinoma, uterine corpus endometrial carcinoma, sarcoma, colorectal adenocarcinoma, ovarian serous cystadenocarcinoma, head and neck squamous cell carcinoma, prostate adenocarcinoma, uterine carcinosarcoma, breast invasive carcinoma, adrenocortical carcinoma, cervical squamous cell carcinoma and endocervical adenocarcinoma, glioblastoma multiforme, renal papillary cell carcinoma, lymphoid neoplasm diffuse large B-cell lymphoma, renal chromophobe, hepatocellular carcinoma, acute myeloid leukemia, pancreatic adenocarcinoma, brain lower grade glioma, renal clear cell carcinoma, and thyroid carcinoma. Ratios were generated using the number of cases altered by each mechanism divided by the total number of cases examined in each cancer that contain the specific alteration.
PTPRT is the most frequently mutated PTPR in human cancers. Wang et al.[13] reported that PTPRT was mutated in 27% of colorectal cancers (CRCs), 17% of gastric cancers, and 18% of lung cancers. They tested the functional consequences of 5 mutations in the catalytic domains of PTPRT and all 5 showed reduced phosphatase activity compared with wild-type PTPRT, indicating that these are loss-of-function mutations[13]. PTPRT mutation has also been reported in other cancers including head and neck squamous cell carcinoma (HNSCC)[14], acute myeloid leukemia[15], and T-cell large granular lymphocytic[16]. Functional analysis of PTPRT mutation in HNSCC revealed that normal function, signal transducer and activator of transcription 3 (STAT3) dephosphorylation, was abrogated for the mutant protein[17].
PTPRD is the second most commonly mutated PTPR across all human cancers. PTPRD mutation has been reported in cutaneous squamous cell carcinoma[18], glioblastoma multiforme (GBM)[19], melanoma[19], CRC[20], HNSCC[14], and lung cancer[21,22]. Functional studies of PTPRD mutation in neuroblastoma, melanoma, and GBM showed that mutation inactivated the function of PTPRD and that cancer cells harboring PTPRD mutations displayed decreased viability, thus suggesting PTPRD acts as a tumor suppressor in these cancers[19,23,24]. Wang et al.[13] also reported 6 (3%) PTPRF mutations in CRCs, 1 (9%) in lung cancer, and 1 (9%) in breast cancer. PTPRF mutation was also reported in HNSCC[14].
Behjati et al.[25] reported 14 PTPRB mutations in 10 of the 39 angiosarcomas studied. In tumors that were secondary and/or had MYC amplification, which is a radiation-associated biomarker of secondary angiosarcoma, the PTPRB mutation rate was up to 45% (10 of 22 cases). PTPRB inhibits angiogenesis, and inactivating mutations of PTPRB are considered driver events in angiosarcoma.
Copy number loss/deletion is common in cancers. Homozygous deletion usually contributes to loss of function of tumor suppressor genes. Many PTPRs negatively regulate cell proliferation, migration, and invasion, and homozygous deletion of these PTPRs may contribute to carcinogenesis. One of the most frequently deleted PTPRs is PTPRD. Homozygous or heterozygous loss of this gene has been reported in cutaneous squamous cell carcinoma[18,26], GBM[19,24], lung cancer[21,27], metastatic melanoma[28,29], neuroblastoma[30], squamous cell carcinoma of the vulva[31], hepatocellular carcinoma[32], and laryngeal squamous cell carcinoma[33] In addition, PTPRF deletion was reported in pheochromocytomas[34]. Down-regulation of PTPRF, considered a tumor suppressor in many cancers, was reported in liver cancer, gastric cancer, and CRC[35].
Promoter methylation is an epigenetic mechanism of regulating gene expression. Tumor suppressors are often silenced by promoter hypermethylation in cancer. Promoter methylation is also an important mechanism for PTPR inactivation in cancer. PTPRG is hypermethylated in multiple cancers including breast cancer[36], gastric cancer[37], nasopharyngeal carcinoma[38], Lynch syndrome CRC[39], childhood acute lymphoblastic leukemia[40], and cutaneous T-cell lymphoma[41]. PTPRG expression is negatively correlated with methylation, and when treated with methylation-suppressive agents like 5-aza-2′-deoxycytidine, PTPRG expression can be recovered[37,41]. A study of childhood acute lymphoblastic leukemia suggested that PTPRG methylation is induced by Ras mutations[40]
Promoter hypermethylation is also the primary mechanism of PTPRO dysregulation. PTPRO hypermethylation has been reported in hepatocellular carcinoma[42,43] colon cancer[44], lung cancer[45], and chronic lymphocytic leukemia[46]. You et al.[47] explored the potential of PTPRO as a biomarker in esophageal squamous cell carcinoma. They found PTPRO methylation in 75.0% (27 of 36) of solid tumors and 36.1%o (13 of 36) of matched peripheral blood samples, whereas no PTPRO methylation was observed in normal peripheral blood from 10 healthy subjects, suggesting PTPRO methylation is an epigenetic biomarker for noninvasive diagnosis of esophageal squamous cell carcinoma[47]. A study of breast cancer showed that PTPRO methylation was associated with lymph node involvement (P = 0.014), poorly differentiated histology (P = 0.037), depth of invasion (P = 0.004), and HER2 amplification (P = 0.001)[48]. PTPRO methylation was detected in 54% (53 of 98) of breast tumors and 34% (33 of 98) of matched peripheral blood samples from patients with breast cancer but in none of the normal peripheral blood samples from 30 healthy individuals[48]. Taken together, PTPRO methylation may represent a biomarker for noninvasive diagnosis and a prognostic factor in breast cancer.
Other PTPRs reported to be hypermethylated in cancer include PTPRD, PTPRF, PTPRJ, PTPRM, PTPRR, PTPRT, and PTPRZ1. In particular, PTPRD was found to be methylated in CRC, breast cancer, HNSCC, and GBM[24]. PTPRF hypermethylation is associated with phenobarbital-induced liver tumorigenesis[49], whereas PTPRJ hypermethylation was induced by microduplications in 2 patients with early-onset CRC[50]. Moreover, Laczmanska et al.[51] reported hypermethylation of PTPRM, PTPRR, PTPRT, and PTPRZ1 in sporadic CRC compared to non-cancer people.
Copy number amplification generally leads to gene overexpression and protein activation and is a common genetic alteration of oncogenes. Several PTPR genes, including PTPRC, PTPRR, and PTPRQ, are reportedly amplified in human cancers. PTPRC has the highest proportion of copy number amplifications among the PTPR genes, based on data for all cancers in the TCGA database. More specifically, PTPRC is amplified in 4.1% (212 of 5,130) of tumor samples across 16 cancers including 11.2% (108 of 962) of breast cancer samples and 13.6% (27 of 199) of liver cancer samples. PTPRQ and PTPRR amplifications were detected in a respective 8.7% (13 of 150) and 17.3% (26 of 150) of sarcoma samples in the TCGA repository. Furthermore, in samples in the TCGA repository, melanomas, lung adenocarcinomas, and sarcomas with PTPRR copy number amplifications have higher PTPRR mRNA levels than samples without copy number amplifications (Figure 2 ).

Protein tyrosine phosphatase receptor type R (PTPRR) amplification Is associated with PTPRR overexpression In lung adenocarcinoma, melanoma, and sarcoma. Unpaired t test was used to compare RNAseq values of TCGA samples with and without copy number changes (CNA), namely, 12 lung adenocarcinoma samples with PTPRR amplification and 126 samples without copy number alteration, 11 melanoma samples with amplification and 231 without copy number alteration, and 19 sarcoma samples with amplification and 53 without copy number alteration. PTPRR mRNA levels were higher in lung adenocarcinomas, melanomas, and sarcomas with amplification compared with those without copy number alterations (respectively, P = 0.0009, P < 0.0001, P = 0.0428).
PTPRA copy gains have also been reported for some cancers. Junnila et al.[52] conducted an array-based analysis of gene expression and copy number levels using gastric cancer samples and then validated the results using the affinity capture-based transcript analysis (TRAC assay) and real-time quantitative reverse transcription-polymerase chain reaction (qRT-PCR). In their study, PTPRA copy number gain was detected in 5 of 13 primary gastric tumors and 3 of 7 gastric cell lines, and PTPRA overexpression was associated with copy number gain. Ardini et al.[53] reported PTPRA overexpression in 29% of breast cancers and found that high expression of PTPRA was associated with low tumor grade and positive estrogen receptor status. Furthermore, PTPRA overexpression in breast cancer cells inhibited cell growth, causing accumulation of cells in G0 or G1 phase[53].
Other PTPR genes that gain copies in cancer include PTPRF and PTPRH. PTPRF amplification was reported in a small cell lung cancer cell line and has also been observed in liver cancer[18,54]. PTPRH is also overexpressed in CRC[55]. Seo et al.[55] found no PTPRH expression in normal colon tissue but detected overexpression in 11.8% (2 of 17) of adenoma samples and 40% (19 of 48) of adenocarcinoma samples, suggesting overexpression of PTPRH may occur late in CRC tumorigenesis. Overall, the functional consequences of PTPR gene amplification are not well understood.
In summary, PTPR dysregulation in cancer occurs through several mechanisms. These include mutation, which is the most common mechanism; deletion and promoter methylation, which cause PTPR inactivation; and gene amplification, though the functional consequences and role of this mechanism require further study.
PTPR Regulation of Cell Signaling in Cancer
PTPRs play important roles in controlling cell signaling. Thus, dysregulation of PTPRs leads to signaling alterations.
Cell proliferation, apoptosis, and survival
PTPRA was reported to dephosphorylate c-Src at inhibitory site Y527, thereby inactivating the protein[56]. Ardini et al.[53] reported that PTPRA overexpression in breast cancer cells inhibited cell growth and caused cells to accumulate in G0 and G1 phase, suggesting PTPRA plays a tumor suppressor role in breast cancer. In estrogen-receptor-negative breast cancer cell lines as well as colon cancer cell lines, siRNA-mediated knockdown of PTPRA reduced Src activity and induced apoptosis[57]. Meyer et al.[58] found that inhibition of PTPRA reduced the growth of HER2-positive breast cancer cells and decreased Akt phosphorylation.
PTPRA is also an important regulator of cell signaling. PTPRE protein dephosphorylates the C-terminal inhibitory sites of Src, Yes, and Fyn, leading to activation of Src family kinases[59]. Further analysis by Kraut-Cohen et al.[60] reveals that, in the absence of activated HER2, PTPRE inhibits the activity of Shc and thus indirectly inhibits the mitogen-activated protein kinase (MAPK) pathway. However, in the presence of HER2, HER2 binds to the PTB domain of Shc and blocks the interaction of PTPRE to Shc, leading to Src activation[60].
PTPRA was reported to regulate a candidate tumor suppressor, death-associated receptor kinase (DARK), at pY491/492 coordinately with Src by dephosphorylating or phosphorylating DARK[61]. In a study in hepatoma cells, Bera et al.[35] found that cell-cell contact during cell proliferation activated PTPRF, which in turn inhibited extracellular related kinase (ERK)-dependent signaling. In prostate cancer, overexpression of PTPRF decreased cell survival, inhibited insulin-like growth factor-1 receptor (IGF-1R) phosphorylation, and enhanced poly (ADP-ribose) polymerase (PARP) cleavage in the presence of neuroendocrine-derived medium[62].
A study of PTPRG’s role as a tumor suppressor revealed that PTPRG inhibited breast tumor formation in vivo and that PTPRG up-regulated p21cip and p27kip proteins through the ERK1/2 pathway in a breast cancer cell model[36]. In nasopharyngeal carcinoma, overexpression of PTPRG suppressed tumor growth in vivo. PTPRG also induced G0/G1 phase arrest through down-regulation of cyclin D1 and stabilization of pRB[38]. Furthermore, PTPRG is considered a tumor suppressor in chronic myeloid leukemia. In addition to interacting with breakpoint cluster region/ABL proto-oncogene 1, non-receptor tyrosine kinase (BCR/ABL) and v-crk avian sarcoma virus CT10 oncogene homolog-like (CRKL) through its intracellular domain, PTPRG, when overexpressed, inhibited BCR/ABL-dependent signaling, whereas down-regulation of PTPRG increased colony formation in chronic myeloid leukemia models[63].
PTPRH affects signaling events related to cell proliferation, apoptosis, and survival. Takada et al.[64] reported that PTPRH induced apoptotic cell death by at least two potential mechanisms, based on their results using a fibroblast cell line model: inhibiting Akt and integrin-linked kinases, which are both downstream of phosphoinositide 3-kinase (PI3K), and activating caspase activity.
PTPRJ regulates Src activity. Namely, after phosphorylation at Y1311 and Y1320 in a Src- and Fyn-dependent manner, PTPRJ then dephosphorylated the Y529 inhibitory site of Src, activated it, and caused vascular endothelial growth factor (VEGF)-induced phosphorylation of vascular endothelial (VE)-cadherin and cortactin[65,66].
In contrast to PTPRJ, PTPRB suppresses angiogenesis by dephosphorylating VEGFR-2 and VE-cadherin and by inhibiting angio-genesis-related signaling[25,67].
STAT3 is an important regulator of cell proliferation and survival. Two PTPRs regulate STAT3 phosphorylation at Y705. When mutated, deleted, or hypermethylated in cancer, PTPRT and PTPRD drive hyperactivation of STAT3, which is accompanied by cell proliferation and, likely, migration in multiple cancers[17,68–71].
Migration, invasion, and metastasis
PTPRA is reported to interact with focal adhesion kinase (FAK) at Y407 in breast cancer[72]. Suppression of PTPRA resulted in increases in FAK phosphorylation, formation of new focal adhesion kinase complexes, and increases in migration. Using colon cancer cells as a model, Krndija et al.[73] found that PTPRA expression is required for invasion into the chorioallantoic membrane.
Overexpression of PTPRF inhibited β-catenin phosphorylation and reduced epithelial cell migration. Overexpression of PTPRF also inhibited tumor formation in nude mice[74]. PTPRF has been implicated to connect noninfiltrating GBM tumor cells to the extracellular glycosylated chondroitin sulfate proteoglycans (CSPGs) which serve as the central organizer of GBM tumor microenvironment. Those glycolsylated CSPGs are absent in the infiltrating GBM tumor cells[75].
PTPRH also plays an important role in migration. Expression of PTPRH induced dephosphorylation of p130cas, a focal adhesion-associated phosphotyrosyl protein, as well as FAK and p62dok in the integrin signaling pathway. Overexpression of PTPRH disrupted the actin-based cytoskeleton and inhibited various integrin-promoted signaling processes[76].
Overexpression of PTPRJ decreased platelet-derived growth factor receptor (PDGFR) signaling by dephosphorylation and inhibition of the MAPK pathway. However, PTPRJ overexpression also caused a redistribution of cadherin and β-catenin, which results in aberrant cell-substratum interactions[77].
In conclusion, PTPR alterations collectively play an important role in modulating cell signaling, leading to effects on proliferation, apoptosis, survival, migration, invasion, and metastasis.
Clinical Implications
Few drugs available to date directly target PTPRs. Several studies have investigated the clinical implication of PTPRs in the setting of cancer treatment. PTPRC is reportedly related to response to radiotherapy in the NCI-60 cancer cell collection[78] A recent report describes a 7-gene signature that predicts relapse and survival for early stage cervical carcinoma, namely PTPRF, ubiquitin-like 3 (UBL3), fibroblast growth factor 3 (FGF3), BMI1 proto-oncogene, polycomb ring finger (BMI1), platelet-derived growth factor receptor, alpha polypeptide (PDGFRA), replication factor C (activator 1) 4 (RFC4), and nucleolar protein 7 (NOL7)[79]. Recurrence-free survival was worse for patients with the signature compared with those without[79]. Notably, because PTPRF controls β-catenin signaling, the PTPRF extracellular domain was studied and confirmed as a novel plasma or tissue-based biomarker in prostate cancer[80].
PTPRF inhibitors are currently in development. Yang et al.[81] used a high-throughput screening assay to identify potential inhibitors of the PTPRF D1 and found that 1 of the 8 candidates showed specificity to PTPRF and was an effective inhibitor. Ajay et al.[82] used in silico assays, including pharmacophore mapping and 3D database searching, followed by SADMET-based virtual screening, docking analysis, and toxicity studies, and discovered 8 nontoxic PTPRF inhibitors. PTPRJ’s tumor suppressor role has been investigated in many human cancers including breast cancer[83], pancreatic cancer[84], and colon cancer[85]. Paduano et al.[86] identified from a phage display library a PTPRJ agonist peptide that binds and activates PTPRJ, leading to reduced MAPK phosphorylation, increased protein level of cell cycle inhibitor p27Kip1, reduced proliferation, and increased apoptosis. Ortuso et al.[87] also discovered a PTPRJ agonist peptide, PTPRJ-pep19.4, and determined that the peptide inhibited in vitro tube formation, ERK1/2 phosphorylation, and proliferation in breast cancer cells but had no effect on primary normal human mammary endothelial cells.
Although there is limited clinical data on drugs that directly target PTPRs, PTPRs have been investigated as biomarkers for treatment or prognosis in different cancers. In addition, PTPR inhibitors and agonists are under development. Challenges in the development of PTPR-targeted therapies include the homology of PTPR catalytic domains[12] and the susceptibility of the active site of most PTPRs to oxidation. Further research is needed on the effect of current and emerging drugs in vivo.
In conclusion, PTPRs are a group of PTPs that share great structural similarity and play key roles in cell signaling. Alterations of these phosphatases, whether by mutation, deletion, amplification, or promoter methylation, are reported to cause aberrations in crucial cellular pathways related to proliferation, apoptosis, survival, migration, and invasion, suggesting these PTPRs are critical components in carcinogenesis. Therefore, efforts to determine how best to target PTPRs are warranted.
References
Charbonneau H, Tonks NK, Kumar S, et al. Human placenta protein-tyrosine-phosphatase: amino acid sequence and relationship to a family of receptor-like proteins. Proc Natl Acad Sci U S A, 1989,86:5252–5256.
Czernilofsky AP, Levinson AD, Varmus HE, et al. Nucleotide sequence of an avian sarcoma virus oncogene (src) and proposec amino acid sequence for gene product. Nature, 1980,287:198–203.
Guan KL, Haun RS, Watson SJ, et al. Cloning and expression of a protein-tyrosine-phosphatase. Proc Natl Acad Sci U S A, 1990,87:1501–1505.
Alonso A, Sasin J, Bottini N, et al. Protein tyrosine phosphatases in the human genome. Cell, 2004,117:699–711.
Buist A, Zhang YL, Keng YF, et al. Restoration of potent protein-tyrosine phosphatase activity into the membrane-distal domain of receptor protein-tyrosine phosphatase alpha. Biochemistry, 1999,38:914–922.
Blanchetot C, Tertoolen LG, Overvoorde J, et al. Intra- and intermolecular interactions between intracellular domains of receptor protein-tyrosine phosphatases. J Biol Chem, 2002,277:47263–47269.
Bilwes AM, den Hertog J, Hunter T, et al. Structural basis for inhibition of receptor protein-tyrosine phosphatase-alpha by dimerization. Nature, 1996,382:555–559.
Nam HJ, Poy F, Saito H, et al. Structural basis for the function and regulation of the receptor protein tyrosine phosphatase CD45. J Exp Med, 2005,201:441–452.
Nam HJ, Poy F, Krueger NX, et al. Crystal structure of the tandem phosphatase domains of RPTP LAR. Cell, 1999,97:449–457.
Salmeen A, Barford D. Functions and mechanisms of redox regulation of cysteine-based phosphatases. Antioxid Redox Signal, 2005,7:560–577.
Salmeen A, Andersen JN, Myers MP, et al. Redox regulation of protein tyrosine phosphatase 1B involves a sulphenyl-amide intermediate. Nature, 2003,423:769–773.
Julien SG, Dube N, Hardy S, et al. Inside the human cancer tyrosine phosphatome. Nat Rev Cancer, 2011,11:35–49.
Wang Z, Shen D, Parsons DW, et al. Mutational analysis of the tyrosine phosphatome in colorectal cancers. Science, 2004,304:1164–1166.
Stransky N, Egloff AM, Tward AD, et al. The mutational landscape of head and neck squamous cell carcinoma. Science, 2011,333:1157–1160.
Becker H, Yoshida K, Blagitko-Dorfs N, et al. Tracing the development of acute myeloid leukemia in CBL syndrome. Blood, 2014,123:1883–1886.
Andersson EI, Rajala HL, Eldfors S, et al. Novel somatic mutations in large granular lymphocytic leukemia affecting the STAT-pathway and T-cell activation. Blood Cancer J, 2013,3:e168.
Lui VW, Peyser ND, Ng PK, et al. Frequent mutation of receptor protein tyrosine phosphatases provides a mechanism for STAT3 hyperactivation in head and neck cancer. Proc Natl Acad Sci U S A, 2014,111:1114–1119.
Lambert SR, Harwood CA, Purdie KJ, et al. Metastatic cutaneous squamous cell carcinoma shows frequent deletion in the protein tyrosine phosphatase receptor type D gene. Int J Cancer, 2012,131:E216–E226.
Solomon DA, Kim JS, Cronin JC, et al. Mutational inactivation of PTPRD in glioblastoma multiforme and malignant melanoma. Cancer Res, 2008,68:10300–10306.
Sjoblom T, Jones S, Wood LD, et al. The consensus coding sequences of human breast and colorectal cancers. Science, 2006,314:268–274.
Kohno T, Otsuka A, Girard L, et al. A catalog of genes homozygously deleted in human lung cancer and the candidacy of PTPRD as a tumor suppressor gene. Genes Chromosomes Cancer, 2010,49:342–352.
Ding L, Getz G, Wheeler DA, et al. Somatic mutations affect key pathways in lung adenocarcinoma. Nature, 2008,455:1069–1075.
Meehan M, Parthasarathi L, Moran N, et al. Protein tyrosine phosphatase receptor delta acts as a neuroblastoma tumor suppressor by destabilizing the aurora kinase A oncogene. Mol Cancer, 2012,11:6.
Veeriah S, Brennan C, Meng S, et al. The tyrosine phosphatase PTPRD is a tumor suppressor that is frequently inactivated and mutated in glioblastoma and other human cancers. Proc Natl Acad Sci U S A, 2009,106:9435–9440.
Behjati S, Tarpey PS, Sheldon H, et al. Recurrent PTPRB and PLCG1 mutations in angiosarcoma. Nat Genet, 2014,46:376–379.
Purdie KJ, Lambert SR, Teh MT, et al. Allelic imbalances and microdeletions affecting the PTPRD gene in cutaneous squamous cell carcinomas detected using single nucleotide polymorphism microarray analysis. Genes Chromosomes Cancer, 2007,46:661–669.
Zhao X, Weir BA, LaFramboise T, et al. Homozygous deletions and chromosome amplifications in human lung carcinomas revealed by single nucleotide polymorphism array analysis. Cancer Res, 2005,65:5561–5570.
Stark M, Hayward N. Genome-wide loss of heterozygosity and copy number analysis in melanoma using high-density single-nucleotide polymorphism arrays. Cancer Res, 2007,67:2632–2642.
Dutton-Regester K, Aoude LG, Nancarrow DJ, et al. Identification of TFG (TRK-fused gene) as a putative metastatic melanoma tumor suppressor gene. Genes Chromosomes Cancer, 2012,51:452–461.
Stallings RL, Nair P, Maris JM, et al. High-resolution analysis of chromosomal breakpoints and genomic instability identifies PTPRD as a candidate tumor suppressor gene in neuroblastoma. Cancer Res, 2006,66:3673–3680.
Micci F, Panagopoulos I, Haugom L, et al. Genomic aberration patterns and expression profiles of squamous cell carcinomas of the vulva. Genes Chromosomes Cancer, 2013,52:551–563.
Nalesnik MA, Tseng G, Ding Y, et al. Gene deletions and amplifications in human hepatocellular carcinomas: correlation with hepatocyte growth regulation. Am J Pathol, 2012,180:1495–1508.
Giefing M, Zemke N, Brauze D, et al. High resolution ArrayCGH and expression profiling identifies PTPRD and PCDH17/PCH68 as tumor suppressor gene candidates in laryngeal squamous cell carcinoma. Genes Chromosomes Cancer, 2011,50:154–166.
Aarts M, Dannenberg H, deLeeuw RJ, et al. Microarray-based CGH of sporadic and syndrome-related pheochromocytomas using a 0.1–0.2 Mb bacterial artificial chromosome array spanning chromosome arm 1p. Genes chromosomes Cancer, 2006,45:83–93.
Bera R, Chiou CY, Yu MC, et al. Functional genomics identified a novel protein tyrosine phosphatase receptor type F-mediated growth inhibition inhepatocarcinogenesis. Hepatology, 2014,59:2238–2250.
Shu ST, Sugimoto Y, Liu S, et al. Function and regulatory mechanisms of the candidate tumor suppressor receptor protein tyrosine phosphatase gamma (PTPRG) in breast cancer cells. Anticancer Res, 2010,30:1937–1946.
Wang JF, Dai DQ. Metastatic suppressor genes inactivated by aberrant methylation in gastric cancer. World J Gastroenterol, 2007,13:5692–5698.
Cheung AK, Lung HL, Hung SC, et al. Functional analysis of a cell cycle-associated, tumor-suppressive gene, protein tyrosine phosphatase receptor type G, in nasopharyngeal carcinoma. Cancer Res, 2008,68:8137–8145.
van Roon EH, de Miranda NF, van Nieuwenhuizen MP, et al. Tumour-specific methylation of PTPRG intron 1 locus in sporadic and Lynch syndrome colorectal cancer. EurJ Hum Genet, 2011,19:307–312.
Xiao J, Lee ST, Xiao Y, et al. PTPRG inhibition by DNA methylation and cooperation with RAS gene activation in childhood acute lymphoblastic leukemia. Int J Cancer, 2014,135:1101–1109.
van Doorn R, Zoutman WH, Dijkman R, et al. Epigenetic profiling of cutaneous T-cell lymphoma: promoter hypermethylation of multiple tumor suppressor genes including BCL7a, PTPRG, and p73. J Clin Oncol, 2005,23:3886–3896.
Motiwala T, Ghoshal K, Das A, et al. Suppression of the protein tyrosine phosphatase receptor type O gene (PTPRO) by methylation in hepatocellular carcinomas. Oncogene, 2003,22:6319–6331.
Hsu SH, Motiwala T, Roy S, et al. Methylation of the PTPRO gene in human hepatocellular carcinoma and identification of VCP as its substrate. J Cell Biochem, 2013,114:1810–1818.
Mori Y, Yin J, Sato F, et al. Identification of genes uniquely involved in frequent microsatellite instability colon carcinogenesis by expression profiling combined with epigenetic scanning. Cancer Res, 2004,64:2434–2438.
Motiwala T, Kutay H, Ghoshal K, et al. Protein tyrosine phosphatase receptor-type O (PTPRO) exhibits characteristics of a candidate tumor suppressor in human lung cancer. Proc Natl Acad Sci U S A, 2004,101:13844–13849.
Motiwala T, Majumder S, Kutay H, et al. Methylation and silencing of protein tyrosine phosphatase receptor type O in chronic lymphocytic leukemia. Clin Cancer Res, 2007,13:3174–3181.
You YJ, Chen YP, Zheng XX, et al. Aberrant methylation of the PTPRO gene in peripheral blood as a potential biomarker in esophageal squamous cell carcinoma patients. Cancer Lett, 2012,315:138–144.
Li SY, Li R, Chen YL, et al. Aberrant PTPRO methylation in tumor tissues as a potential biomarker that predicts clinical outcomes in breast cancer patients. BMC Genet, 2014,15:67.
Phillips JM, Goodman JI. Identification of genes that may play critical roles in phenobarbital (PB)-induced liver tumorigenesis due to altered DNA methylation. Toxicol Sci, 2008,104:86–99.
Venkatachalam R, Ligtenberg MJ, Hoogerbrugge N, et al. Germline epigenetic silencing of the tumor suppressor gene PTPRJ in early-onset familial colorectal cancer. Gastroenterology, 2010,139:2221–2224.
Laczmanska I, Karpinski P, Bebenek M, et al. Protein tyrosine phosphatase receptor-like genes are frequently hypermethylated in sporadic colorectal cancer. J Hum Genet, 2013,58:11–15.
Junnila S, Kokkola A, Karjalainen-Lindsberg ML, et al. Genomewide gene copy number and expression analysis of primary gastric tumors and gastric cancer cell lines. BMC Cancer, 2010,10:73.
Ardini E, Agresti R, Tagliabue E, et al. Expression of protein tyrosine phosphatase alpha (RPTPalpha) in human breast cancer correlates with low tumor grade, and inhibits tumor cell growth in vitro and in vivo. Oncogene, 2000,19:4979–4987.
Harder KW, Saw J, Miki N, et al. Coexisting amplifications of the chromosome 1p32 genes (PTPRF and MYCL1) encoding protein tyrosine phosphatase LAR and L-myc in a small cell lung cancer line. Genomics, 1995,27:552–553.
Seo Y, Matozaki T, Tsuda M, et al. Overexpression of SAP-1, a transmembrane-type protein tyrosine phosphatase, in human colorectal cancers. Biochem Biophys Res Commun, 1997,231:705–711.
Su J, Muranjan M, Sap J. Receptor protein tyrosine phosphatase alpha activates Src-family kinases and controls integrin-mediated responses in fibroblasts. Curr Biol, 1999,9:505–511.
Zheng X, Resnick RJ, Shalloway D. Apoptosis of estrogen-receptor negative breast cancer and colon cancer cell lines by PTP alpha and src RNAi. Int J Cancer, 2008,122:1999–2007.
Meyer DS, Aceto N, Sausgruber N, et al. Tyrosine phosphatase PTPalpha contributes to HER2-evoked breast tumor initiation and maintenance. Oncogene, 2014,33:398–402.
Granot-Attas S, Elson A. Protein tyrosine phosphatase epsilon activates Yes and Fyn in Neu-induced mammary tumor cells. Exp Cell Res, 2004,294:236–243.
Kraut-Cohen J, Muller WJ, Elson A. Protein-tyrosine phosphatase epsilon regulates Shc signaling in a kinase-specific manner: increasing coherence in tyrosine phosphatase signaling. J Biol Chem, 2008,283:4612–4621.
Wang WJ, Kuo JC, Ku W, et al. The tumor suppressor DAPK is reciprocally regulated by tyrosine kinase Src and phosphatase LAR. Mol Cell, 2007,27:701–716.
DaSilva JO, Amorino GP, Casarez EV, et al. Neuroendocrine-derived peptides promote prostate cancer cell survival through activation of IGF-1R signaling. Prostate, 2013,73:801–812.
Della Peruta M, Martinelli G, Moratti E, et al. Protein tyrosine phosphatase receptor type (gamma) is a functional tumor suppressor gene specifically downregulated in chronic myeloid leukemia. Cancer Rres, 2010,70:8896–8906.
Takada T, Noguchi T, Inagaki K, et al. Induction of apoptosis by stomach cancer-associated protein-tyrosine phosphatase-1. J Biol Chem, 2002,277:34359–34366.
Chabot C, Spring K, Gratton JP, et al. New role for the protein tyrosine phosphatase DEP-1 in akt activation and endothelial cell survival. Mol Cell Biol, 2009,29:241–253.
Spring K, Chabot C, Langlois S, et al. Tyrosine phosphorylation of DEP-1/CD148 as a mechanism controlling Src kinase activation, endothelial cell permeability, invasion, and capillary formation. Blood, 2012,120:2745–2756.
Hayashi M, Majumdar A, Li X, et al. VE-PTP regulates VEGFR2 activity in stalk cells to establish endothelial cell polarity and lumen formation. Nat Commun, 2013,4:1672.
Veeriah S, Brennan C, Meng S, et al. The tyrosine phosphatase PTPRD is a tumor suppressor that is frequently inactivated and mutated in glioblastoma and other human cancers. Proc Natl Acad Sci U S A, 2009,106:9435–9440.
Ortiz B, Fabius AW, Wu WH, et al. Loss of the tyrosine phosphatase PTPRD leads to aberrant STAT3 activation and promotes gliomagenesis. Proc Natl Acad Sci U S A, 2014,111:8149–8154.
Qi J, Li N, Fan K, et al. Beta1,6 GlcNAc branches-modified PTPRT attenuates its activity and promotes cell migration by STAT3 pathway. PLoS One, 2014,9:e98052.
Zhang X, Guo A, Yu J, et al. Identification of STAT3 as a substrate of receptor protein tyrosine phosphatase T. Proc Natl Acad Sci U S A, 2007,104:4060–4064.
Boivin B, Chaudhary F, Dickinson BC, et al. Receptor protein-tyrosine phosphatase alpha regulates focal adhesion kinase phosphorylation and ErbB2 oncoprotein-mediated mammary epithelial cell motility. J Biol Chem, 2013,288:36926–36935.
Krndija D, Schmid H, Eismann JL, et al. Substrate stiffness and the receptor-type tyrosine-protein phosphatase alpha regulate spreading of colon cancer cells through cytoskeletal contractility. Oncogene, 2010,29:2724–2738.
Muller T, Choidas A, Reichmann E, et al. Phosphorylation and free pool of beta-catenin are regulated by tyrosine kinases and tyrosine phosphatases during epithelial cell migration. J Biol Chem, 1999,274:10173–10183.
Silver DJ, Siebzehnrubl FA, Schildts MJ, et al. Chondroitin sulfate proteoglycans potently inhibit invasion and serve as a central org anizer of the brain tumor microenvironment. J Neurosci, 2013,33:15603–15617.
Noguchi T, Tsuda M, Takeda H, et al. Inhibition of cell growth and spreading by stomach cancer-associated protein-tyrosine phosphatase-1 (SAP-1) through dephosphorylation of p130cas. J Biol Chem, 2001,276:15216–15224.
Kellie S, Craggs G, Bird IN, et al. The tyrosine phosphatase DEP-1 induces cytoskeletal rearrangements, aberrant cell-substratum interactions and a reduction in cell proliferation. J Cell Sci, 2004,117:609–618.
Kim HS, Kim SC, Kim SJ, et al. Identification of a radiosensitivity signature using integrative metaanalysis of published microarray data for NCI-60 cancer cells. BMC Genomics, 2012,13:348.
Huang L, Zheng M, Zhou QM, et al. Identification of a 7-gene signature that predicts relapse and survival for early stage patients with cervical carcinoma. Med Oncol, 2012,29:2911–2918.
Whitmore TE, Peterson A, Holzman T, et al. Integrative analysis of N-linked human glycoproteomic data sets reveals PTPRF ectodomain as a novel plasma biomarker candidate for prostate cancer. J Proteome Res, 2012,11:2653–2665.
Yang X, Li J, Zhou Y, et al. Discovery of novel inhibitor of human leukocyte common antigen-related phosphatase. Biochim Biophys Acta, 2005,1726:34–41.
Ajay D, Sobhia ME. Identification of novel, less toxic PTP-LAR inhibitors using in silico strategies: pharmacophore modeling, SADMET-based virtual screening and docking. J Mol Model, 2012,18:187–201.
Keane MM, Lowrey GA, Ettenberg SA, et al. The protein tyrosine phosphatase DEP-1 is induced during differentiation and inhibits growth of breast cancer cells. Cancer Res, 1996,56:4236–4243.
Trapasso F, Yendamuri S, Dumon KR, et al. Restoration of receptor-type protein tyrosine phosphatase eta function inhibits human pancreatic carcinoma cell growth in vitro and in vivo. Carcinogenesis, 2004,25:2107–2114.
Luo L, Shen GQ, Stiffler KA, et al. Loss of heterozygosity in human aberrant crypt foci (ACF), a putative precursor of colon cancer. Carcinogenesis, 2006,27:1153–1159.
Paduano F, Ortuso F, Campiglia P, et al. Isolation and functional characterization of peptide agonists of PTPRJ, a tyrosine phosphatase receptor endowed with tumor suppressor activity. ACS Chem Biol, 2012,7:1666–1676.
Ortuso F, Paduano F, Carotenuto A, et al. Discovery of PTPRJ agonist peptides that effectively inhibit in vitro cancer cell proliferation and tube formation. ACS Chem Biol, 2013,8:1497–1506.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Du, Y., Grandis, J.R. Receptor-type protein tyrosine phosphatases in cancer. Chin J Cancer 34, 61–69 (2015). https://doi.org/10.5732/cjc.014.10146
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.5732/cjc.014.10146